1). “Republicans Aren't Done With Mifepristone: Here's what happens next”, May 15, 2026, Jessica Valenti & Kylie Cheung, Abortion, Every Day, at < https://jessica.substack.com/
2). “SCOTUS Kicks Mife Back to Lower Court—Access Remains”, May 14, 2026, Jessica Valenti & Kylie Cheung, Abortion, Every Day, at at < https://jessica.substack.com/
3). “The Biggest Attack on Abortion Since the End of Roe: A federal court wants to end mifepristone by mail—it's not happening”, May 02, 2026, Jessica Valenti, Abortion, Every Day, at < https://jessica.substack.com/
4). “Shield Laws for Reproductive and Gender-Affirming Health Care: A State Law Guide”, Updated Mar 2026, Anon, UCLA Law, Shield Law Scholarship, at < https://law.ucla.edu/
5). “The History of Mifepristone”, Apr 18, 2023 (Updated Mar 27, 2024), Anon, Reproductive Health Access Project, at < https://www.
6). “Do 1 in 5 women suffer complications from abortion pills? No. Group suing FDA shares flawed data.”, April 13, 2023, Samantha Putterman, Politifact, Poynter Institute, at < https://www.politifact.com/
7). “Abortion pills by mail surge despite Texas' bans. How long can it last? | Opinion”, Updated Jan 16, 2025, Bridget Grumet, Austin American-Statesman, at < https://www.statesman.com/
8). “New Gov't Website Will Help Collect CPCs Data On Pregnant Women”, May 11, 2026, Jessica Valenti, Abortion, Every Day, at < https://jessica.substack.com/
9). “Missouri ‘born-alive’ abortion bill heads to governor after contentious House debate: Under the ‘Born-Alive Abortion Survivors Protection Act,’ anyone who ‘knowingly performs or attempts to perform an overt act that kills a child born alive’ can be charged with first-degree murder”, May 13, 2026, Anna Spoerre, Missouri Independent, at < https://missouriindependent.
~~ recommended by desmond ~~
Introduction by desmond: While Trump is busy stealing $1.7 Billion of taxpayer funds with which to reward his ground troops in the Proud Boys and Oathkeepers and other far right-wing militias; his allies in the The Forced-Pregnancy / Forced-Birth movement are busy trying to impose the harsh Dark Ages Red States laws against abortions on the enlightened and still protected Blue States. Even more of a target of the Far-Right's Forced-Pregnancy / Forced-Birth movement are the medical professionals who assist women who live in the Dark Ages Red States by sending them Mifepristone and Misoprostol through the mail.
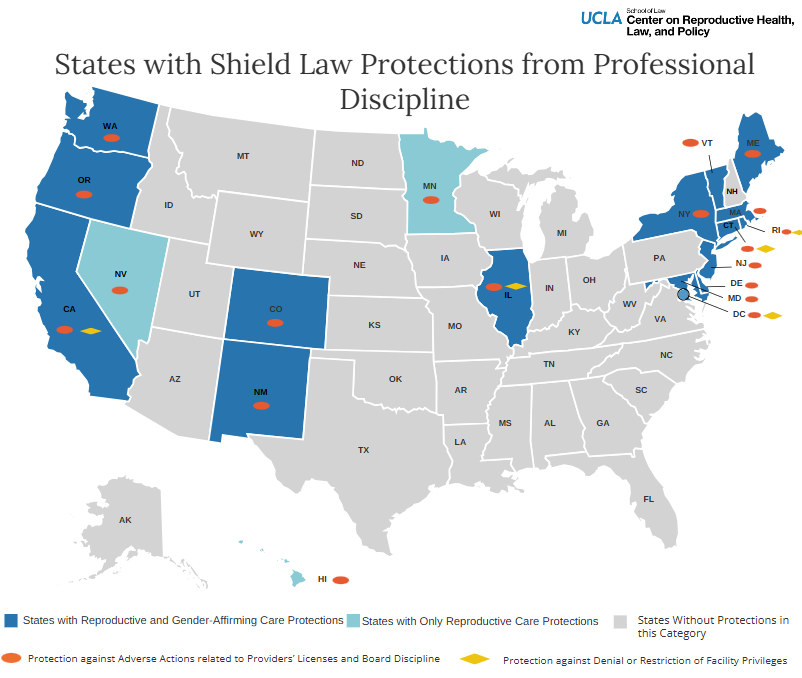
Jessica Valenti and Kylie Cheung, in Item 1)., “Republicans Aren't Done ….”; Item 2)., “SCOTUS Kicks Mife ….”; and Item 3)., “The Biggest Attack ….”, discuss various ramifications of the situation now that the most reactionary court in the U.S. (the Fifth Circuit Appeals Court), that presides over Texas, Mississippi, and Louisiana, has issued a stay attempting to end tele-medicine operations that provide Mifepristone and Misoprostol to women seeking medication abortions. These providers are protected by a variety of Shield Laws, in the 22 States and the District of Columbia. Item 4)., “Shield Laws for Reproductive ….”, lists the various aspects of the laws passed in those 23 political entities. Most aggressive in defending the activities of those who help women in the Dark Ages Red States are California, Colorado, Maine, Massachusetts, New York State, Rhode Island, Vermont, and Washington State. Those 8 states specifically protect medical personnel working to provide medication abortion, and other services, to women who live in Dark Ages Red States from criminal prosecution or civil penalties. See the U.S. map below for a summary of what the situation is in the 22 Blue States and D.C. Item 4 includes 6 Maps and a useful Table to explain the situation in some detail.

The Forced-Pregnancy / Forced-Birth movement's attorneys and strategists have promoted a totally false image of medication abortion as being dangerous and are now rapidly passing laws making Mifepristone into a controlled substance on the level of Heroin or Morphine with decades of imprisonment for anybody their forces capture who possesses those substances. Item 5)., “The History of Mifepristone” reveals the truth about Mifepristone. It was first synthesized in France in the mid 1980s, and was accepted by France for medication abortion in 1988, and has proven to be a safe medicine. Resistance by the Forced-Pregnancy / Forced-Birth movement in the U.S. delayed Mifepristone's (also known as RU-486) use in the U.S. for a dozen years in 2000. Even then it required a visit to a physician to prescribe medication abortion, and the U.S. far-right has conducted a massive disinformation campaign against Mifepristone ever since it began to be used.
In Item 6)., “Do 1 in 5 women suffer ….”, the article debunks the flawed and deceptive tactics used to try to scare women away from medication abortion. However, the Covid Pandemic, led to the CDC changing regulations and allowing medical practices to prescribe it without an office visit. This was during the Biden Administration. Recently a new bogus study was submitted as An April report from the Ethics and Public Policy Center (EPPC) written by authors associated with the EPPC a far-right Catholic organization. That flawed and deceptive study has been cited in various attacks on medication abortion. The real reason that the Forced-Pregnancy / Forced-Birth movement is opposed to medication abortion is it deprives their thuggish operatives the chance to try to shame and intimidate women arriving at abortion clinics. There is no doubt that medication abortion is a much better alternative for all women in the 27 Dark Ages Red States and even in the 23 Blue States and D.C. See Bar Chart of the growth of medication abortion below.

Item 7)., “Abortion pills by mail ….” profiles medical personnel providing medication abortion to Dark Ages Red States from a Blue State. The main operative profiled in the article stated that she would move overseas and continue providing Mifepristone and Misoprostol from a foreign locale if it becomes too dangerous legally to do so even from a Blue State.
Item 8)., “New Gov't Website ….”, and Item 9)., “Missouri ‘born-alive’ ….”, both discuss the malign and vicious operations of parts of the various governmental agencies that are controlled by either the federal government, as discussed in Item 8, or the far-right Forced-Pregnancy / Forced-Birth movement at the state level. The new website discussed in Item 8, “Moms.gov”, funnels vulnerable women to Option Line, one of the tools that Heartbeat International uses to collect massive amounts of data on pregnant women. Heartbeat International operates numerous Crisis Pregnancy Centers and works with others to try to dissuade women from obtaining abortions and to hopefully delay them until it is too late. The Missouri State law passed by the State Legislature in Item 9)., is another ridiculous attempt at control, that burdens physicians with legal threats for long-terms of imprisonment and heavy fines for doing what is needed for women who have had a difficult late-term pregnancy and who generally have miscarried. Democratic Opponents of the law point out that Missouri has lost 25% of its OB/GYNs since the Trumpian Abortion Bans were passed in 2022. What's more Missouri is having a hard time recruiting OB/GYNs to move there.
xxxxxxxxxxxxxxxxxx
Republicans Aren't Done With Mifepristone
Last night, the Supreme Court kicked telemedicine abortion back down to the Fifth Circuit. That means access to mifepristone by mail remains the same—a clear short-term win that gives advocates and providers some much-needed breathing room.
But in terms of the broader politics and long-term access, the decision was a mixed bag: by returning the case to a lower court, SCOTUS bought precious time for Republicans, who aren’t eager to deal with one of their most unpopular issues before the midterms. Dissents from Justices Samuel Alito and Clarence Thomas also laid out a legal roadmap for conservatives going forward—with Alito arguing that telemedicine abortion undermines the Court’s decision in Dobbs, and Thomas pointing to the Comstock Act.
Like we said last night, this is a reprieve—not a win. After all, the end of Roe caused a fundamental conflict between banned and pro-choice states—one that can’t be punted forever.
In the meantime, the anti-abortion movement—as angry as they are—is getting what they want: chaos, confusion, and American women believing their ability to access abortion pills is entirely dependent on whatever court order is released that day.
So let’s clear some things up and talk about what happens next.
How did we get here?
On May 1, a federal court temporarily blocked the FDA rule that allows mifepristone to be prescribed without an in-person visit. The conservative Fifth Circuit Court of Appeal ruled in favor of a suit brought by Louisiana Attorney General Liz Murrill, who argued that telehealth access to mifepristone is dangerous, that it enables abusers to ‘coerce’ their victims into abortion, and that it harms her Republican state by allowing women to sidestep its ban.
The court agreed that the FDA rules “undermine” Louisiana’s anti-abortion law, setting off a domino effect of fear and confusion.
What happened after the Fifth Circuit ruling?
Almost immediately after the federal court decision came down, media headlines declared that abortion pills by mail were now illegal—even though that wasn’t entirely true. The Fifth Circuit only changed FDA regulatory guidelines, not state or federal law.
The ruling didn’t mean that women would now be arrested or prosecuted for ordering abortion pills by mail. There was also debate among providers about what the ruling meant for them, because the FDA’s enforcement authority is typically directed toward manufacturers and distributors—not providers themselves. That’s why some continued to ship mifepristone per usual, while others switched to miso-only.
All of which is to say, it’s more complicated than the headlines let on. Consider revisiting Abortion, Every Day’s explainer for more clarity:
Soon after the decision came down, Democratic attorneys general and mifepristone manufacturers asked the Supreme Court to intervene. SCOTUS responded by pausing the Fifth Circuit ruling, extending that pause, and then—last night—issuing an order.
In addition to the flurry of legal decisions, there’s been lots of related political maneuvering happening in the background these last few weeks; click here for a run-down.
What are the stakes?
The Court’s decision—and what comes next—has vast implications for abortion rights in every state. Abortion-pills-by-mail—and providers’ ability to ship mifepristone without fear of state reprisal—is propping up access nationwide.
Nearly two-thirds of American abortions are provided using abortion pills, and almost 30% of all abortions are obtained using telehealth. The availability of abortion medication across state lines is one of the primary reasons the national abortion rate has remained steady. And when someone has an abortion in a banned state, it’s almost always a telemedicine abortion.
That’s precisely why Louisiana filed this lawsuit in the first place—not because there are any real ‘safety concerns’ about mifepristone. They’re mad that women are breaking their rules.
Republicans want every single one of us trapped under post-Dobbs bans. That’s why they’re not just targeting abortion pills, but the shield laws that protect the providers who ship them. Their (very explicit) goal is to extradite healthcare providers from pro-choice states and punish them in states where they could get life in prison.

Where is the Trump administration in all this?
Eerily quiet. The Trump administration—understanding how unpopular abortion restrictions are with voters—has mostly steered clear of any big showy moves lately. In fact, the administration even sought a temporary pause on Louisiana’s suit in January, saying the FDA needed time to complete their sham ‘safety study’ of mifepristone.
Anti-abortion activists were not pleased, especially because of reports that former FDA commissioner Marty Makary was slow-walking the bogus study until the midterms. Basically, the administration was using the promise of this study as a way to mollify anti-abortion groups without actually doing anything.
That said, the administration has been keeping its options open: when Trump’s DOJ asked for that pause in the case, for example, they did so on standing—not the merits. In other words, they didn’t dispute any of Louisiana’s false claims about mifepristone; they simply asked the court to delay the case on technical grounds.
As the ACLU Reproductive Freedom Project’s Julia Kaye said at the time, “the Trump administration isn’t defending medication abortion—it’s just defending its own authority to restrict access to mifepristone if, when, and how it sees fit.”
That aligns with what they’re doing now, too. Since the Fifth Circuit ruling, the FDA and Trump administration hasn’t said much of anything; some advocates tell AED the assumption is that the White House is trying to have their cake and eat it too. They don’t want to come out publicly against abortion pills and risk voters’ ire, but want the ability to ban abortion pill access at some point. The real trick is messaging to the anti-abortion movement that they still plan on the latter.
It’s like I pointed out last night: there’s a reason the FDA tweeted about the so-called safety study soon after the order from SCOTUS came down. By promising to “press forward” and “provide greater transparency,” the administration is asking the anti-abortion movement to hold tight.
It’s also not a coincidence that the new acting commissioner of the FDA is doing the rounds with anti-abortion activists: Kyle Diamantas promised Lila Rose of Live Action and Kristan Hawkins from Students for Life that “reviewing the abortion pill is a top priority.” He’s been dispatched to smooth things over, until the administration is ready make a more public move.
What do we do now?
We can’t just sit back and wait for more Trump-appointed judges to attack mifepristone. Telehealth is headed back to the courts, where anti-abortion legal groups and attorneys general will hone their arguments for the next time they go to SCOTUS. They’ve played the long game before, and now is no different. While they’re preparing, so should we.
Order advance provision abortion medication: You all know I’m an advance provision evangelist! Everyone should have abortion pills in their medicine cabinet just in case you—or someone you know—needs it. Especially given that the legal confusion of the past few weeks is sure to repeat itself.
Go to Plan C Pills, I Need An A, or Aid Access to buy pills to have on hand. Abortion, Every Day also has a robust resources page where you can find information on how to get abortion medication, along with legal and medical help.
Keep an eye on the midterms: I’m reminded every single day doing this work why elections matter so much. Look at the courts, ffs! If you have the ability to do some door-knocking or phone-banking ahead of the midterms, now is the time.
And attacks on abortion pills aren’t just happening at the national level. In state after state, Republicans are passing laws to increase penalties associated with having or dispensing abortion pills—in some cases classifying them as controlled substances, or legislating them under ‘drug trafficking’.
Every election matters—national, state, and local. Keep an eye out for more midterms coverage from AED; we’re working on an election guide of sorts that we hope will be useful.
Spread the word about the safety of abortion pills: The anti-abortion movement has been unfortunately successful at pushing out misinformation about abortion medication. (This KFF tracking poll haunts my nightmares.) That’s in large part because they’ve been extraordinarily disciplined about their messaging: whenever an anti-abortion group or activist gives an interview to the media, they’re talking about ‘trafficking’, ‘coercion’, and the supposed danger that mifepristone poses to women.
We need to be just as relentless with the truth.
Support local providers & funds: As you know, the folks making sure that patients get the medication they need are often working on the local level. They’re your friendly neighborhood abortion fund or clinic, and chances are they’re stretched way thin. Donate, volunteer, or reach out to see what help they need most.
Keep independent feminist media alive: Okay, this one is slightly self-serving, but I know you’ll understand. AED is working incredibly hard every day to keep you activated and informed. So many of you already support the newsletter with a paid subscription (thank you!!), but most readers don’t. That’s okay! I don’t support every newsletter I read, either. But if you can swing it, every paying member here really does make a huge difference. You can even sign up now at a discount.
I’ve said it before and I’ll say it again: Republicans want us to feel confused, scared, and alone. Our job is to make sure that doesn’t happen. Abortion pills aren’t going anywhere—not while we’re here taking care of each other.
xxxxxxxxxx
Supreme Court Decision on Mifepristone Sends it Back to Lower Court—Access Stays the Same
Quick hits: Mifepristone Goes Back to the Fifth Circuit; Illinois Bill Would Protect Abortion Records; Arkansas ‘Monument to the Unborn’ is a Stolen Design; In the States: Arizona, Kentucky, Oregon, Missouri, Colorado; Which Pro-Choice States Are Stepping Up for Planned Parenthood?; Virginia Ordinance Sidesteps Abortion Protections
Mifepristone Goes Back to the Fifth Circuit
Well, that very nearly gave me a heart attack! The Supreme Court missed its own 5 p.m. deadline today, allowing a Fifth Circuit ruling targeting mifepristone-by-mail to briefly go into effect. But around 5:30, the Court granted the emergency stay requested by mifepristone manufacturers Danco and GenBioPro. That means abortion pills can continue to be sent by mail while the case works its way back through the lower courts.
The Justices didn’t give an explanation for the decision, or the vote count—just the order itself. What we do know is that Justices Clarence Thomas and Samuel Alito dissented, doing pretty much exactly what you’d expect—laying out how anti-abortion activists and lawyers should come after mifepristone next: Thomas pointed to the Comstock Act, and said mifepristone manufacturers weren’t entitled to a stay “based on lost profits from their criminal enterprise.” (Asshole.) Alito said the companies hadn’t met the legal bar for a stay, and—incredibly—called telemedicine abortion “a scheme to undermine our decision in Dobbs.” (Also an asshole.)
Here’s what happens now: the case goes back to the Fifth Circuit to be decided on the merits. The stay holds through that process—meaning that mifepristone will continue to be available as it is now. But it’s almost certain that this case is going to end up back at the Supreme Court. Several abortion rights leaders tell me they see this as SCOTUS’ way of delaying that inevitability for as long as possible. Or at least until after the midterms.
Keep an eye on your inboxes: tomorrow, Abortion, Every Day will send you a full breakdown of the decision, what it means, and what we do now.
Something to keep an eye on in the meantime: the FDA sent out a tweet tonight about the Supreme Court’s decision—using language meant to seem reasonable, but that actually signals something more insidious.
My take? The FDA is sending a message to the anti-abortion movement: hold tight, the bogus “safety review” of mifepristone is coming. Especially given the new interim FDA chief, who—Reproductive Freedom for All president Mini Timmaraju reminded me—got on the phone with anti-abortion activists this week to assure them he’s on their side!
So let’s take tonight to be relieved: abortion pill access stays the same for right now, and that’s amazing. (Also amazing: anti-abortion activists are pissed off.) But let’s not lose sight of the fact that this is conservatives’ way of kicking the can down the road, and we still have lots of work to do.
Illinois Bill Would Protect Abortion Records
Let’s move on to some objectively terrific news: Illinois Democrats have introduced legislation that would help protect abortion patients’ medical privacy.
The Reproductive Health Records Privacy Act would allow for “segregation of abortion-related information in health information exchanges”—in other words, information related to abortion care would be separated out from other medical records. The bill would also limit the ability of out-of-state entities to access that information; so abortion records would be flagged as protected in routine records requests unless a patient specifically asks for the data to be shared.
State Rep. Mary Beth Canty smartly pointed out to Axios that health issues after a medication abortion can be treated the same as a miscarriage, allowing patients to share as much or as little about their abortion as they wish.
It’s not just an important protection for those in Illinois—but all the abortion patients who come to the state for care. As a reminder, about a quarter of all patients who traveled across state lines for abortion care in 2025 went to Illinois.
Arkansas ‘Monument to the Unborn’ is a Stolen Design
This is just so hilariously on brand. Remember how Arkansas plans to erect a “monument to the unborn” at the state capitol? Well, after years of hand-wringing over designs, the Arkansas Capitol Arts and Grounds Commission finally made a decision—and apparently decided the best way to honor aborted fetuses was to steal from a local artist.
The state panel chose a design submitted by a Republican legislator: a “living wall” of plants. But here’s the thing, artist Lakey Goff submitted that exact concept to the commission years ago—and the panel accepted it. Apparently Republicans thought her version would be too costly, so they rescinded its acceptance and proposed their own smaller and cheaper version.
“There’s corruption and there’s deceit, and this system has got to be accounted for in the name of Jesus,” Goff says. “What they have done is a disgrace, and it is unrighteous, and it is not in alignment with the will of God for the state of Arkansas.”
Obviously I don’t think stealing from artists is okay, but given the subject matter I’m just going to say this: play stupid games, win stupid prizes.
In the States: Arizona, Kentucky, Oregon, Missouri, Colorado
Anti-abortion legislators in Arizona are hiring their own private lawyers to defend state abortion restrictions—even though voters codified protections for abortion in 2024. What’s more, they’re not hiring the lawyers on their own dime. Taxpayers will foot the bill.
This started because a group of advanced practice nurses are challenging a state law that limits who can prescribe or perform abortions. The suit, brought on the nurses’ behalf by the ACLU, points out that the law has nothing to do with patient safety or medical standards—and that it’s more important than ever to expand the state’s pool of providers. (Like all pro-choice states, Arizona has seen an increase in out-of-state patients, and is struggling to meet the demand.)
But here’s the thing: Arizona Attorney General Kris Mayes is pro-choice, and she has no plans to fight the ACLU’s suit. That’s why Republicans are hiring attorneys to push against the challenge themselves.
“To me, the question is, why is the legislature spending taxpayer money to defend these kinds of things in the face of the will of the voters,’‘ Arizona solicitor general Josh Bendor asks. I would love to know the answer!
Meanwhile, Kentucky’s attorney general has asked a judge to reconsider his ruling striking down the state’s definition of human life. Under Kentucky’s abortion ban, human life is defined as beginning at conception, but Jefferson Circuit Judge Brian Edwards called the definition “unconstitutionally void for vagueness.” (The decision came in response to a broader religious freedom challenge to the law.)
Edwards also cited Republican legislation seeking to punish abortion patients with homicide, and a recent case where a Kentucky woman was arrested for fetal homicide after having an abortion.
But Attorney General Russell Coleman insists that the idea that women could be charged for having abortions “is a gross over-reading” of the state ban. “There is…no basis to conclude that the definition of ‘unborn human being’…could ever be used as a basis for a homicide prosecution,” Coleman said.
Tell that to the hundreds of women who’ve been charged with pregnancy-related crimes since the end of Roe!
As expected, Missouri just passed its heinous Born Alive bill that we’ve been covering, now off to the governor’s desk. Dr. Katrina Kimport, a researcher focusing on later abortion care at Advancing New Standards in Reproductive Health (ANSIRH) previously toldAED about a pregnant patient who learned there was no way her child would survive. The woman wanted to give birth and receive palliative care—to spend a few hours with her newborn without medical intervention, in order to say goodbye.
But she lived in a state with ‘Born Alive’ legislation, which required the hospital to intervene to ‘save the baby’s life’—prolonging the infant and family’s suffering. If she fought back against that ‘life-saving’ care, she could be reported to child protective services. (The woman felt forced by the state to travel for later abortion care.)
State Rep. Brian Seitz told the Missouri Independent, “The Democrats are putting themselves in a very dangerous political position by not supporting healthcare for a living child.” But let’s be clear: to Republicans like Seitz, a newly fertilized egg is a “living child.”
In better news, Colorado is one step closer to requiring abortion medication on college campuses. Colorado Newsline reports that a bill requiring campus health centers to keep the medication in stock has passed the legislature and will now head to Gov. Jared Polis for his signature.
The bill would mandate that colleges with pharmacies on campus keep the medication in stock; colleges without pharmacies would still have to send prescriptions for the pills somewhere else.
Bill sponsor Sen. Katie Wallace said in a statement, “College students are navigating a nation that continues to undermine their right to abortion care, but Colorado is and will remain a safe haven for reproductive rights.”
Which Pro-Choice States Are Stepping Up for Planned Parenthood?
Oregon’s governor has signed three new laws to protect and strengthen abortion rights—including one that will backfill Planned Parenthood funding that’s been cut under the Trump administration.
In fact, Jefferson Public Radio points out that thanks to House Bill 4127, Oregon has become the first state to create a long-term plan to replace clinic funding should Congress permanently cut those federal dollars off. Democratic lawmakers have already set aside over $7 million—but that’s less than half of the $17 million clinics needed in 2024.
Gov. Tina Kotek also signed House Bill 4088, which expands the state’s shield law by prohibiting state employees from helping out-of-state or federal investigations into those providing abortions and gender affirming care.
“At a time when reproductive health care is under relentless attack across our country, Oregon chose to lead,” said Amy Handler, the president of Planned Parenthood of Southern Oregon.
Speaking of Planned Parenthood funding, the Detroit Free Press reports that Michigan clinics are in danger of shuttering if the organization doesn’t get $5 million in state funding.
Planned Parenthood of Michigan is asking Gov. Gretchen Whitmer to push through the red tape to get the group emergency funding as soon as possible. In an open letter, president Paula Thornton Greear writes, “Without urgent state action, we will soon be forced to make decisions about our health centers and our programs that cannot be undone.”
Whitmer’s press secretary, Stacey LaRouche, says that getting funding to Planned Parenthood is the legislature’s job. “We would encourage any organization or individual to work with the Legislature on their budget asks,” she told the Detroit Free Press. But Thornton Greear pointed out that other governors—like Illinois Gov. J.B. Pritzker—have managed to go around the normal budgetary process to protect reproductive healthcare in their states.
Consider this yet another reminder that Republicans’ budget bill is meant to be a de facto national ban—if they can’t make abortion illegal in every state, they’ll make it impossible to get. Planned Parenthood has already closed clinics in Jackson, Marquette, and Petoskey, and has consolidated two Ann Arbor centers.
In her letter, Thornton Greear says it plainly to Whitmer:
“Put simply: there is no one else who can act to save our health centers. It is down to you.”
Read more about the Trump administration’s defunding plan in our explainer below:
Virginia Ordinance Sidesteps Abortion Protections
So much for leaving abortion to the states!
Earlier this year, Lynchburg, Virginia passed an ordinance to ban abortion clinics from operating within a thousand feet of churches, public libraries, schools, parks, children’s museums, and day care centers. The list was so long that there would effectively be no place in Lynchburg where a clinic could set up.
Still, the council debated making the ordinance even more extreme this week by potentially removing language that exempts clinics that offer “family planning services,” because council member Chris Faraldi said this could allow “Planned Parenthood [to] set up right across the street from E.C. Glass High School.”
Let’s be clear: there’s nothing inappropriate about a health care center opening near a school or church.
Faraldi claimed that this exception for family planning clinics that don’t provide abortion was about “[ramming the ordinance] through all for political posture in an election year.” Another council member, Marty Misjuns, argued that “the pro-life community in Lynchburg should be proud of what we’ve accomplished in Lynchburg.”
Here’s what these ordinances really are: informal, local abortion bans meant to circumvent state laws. Anti-abortion activists think people won’t pay attention to local politics—and that they can push through restrictions using boring zoning policies without anyone noticing. That’s exactly what makes these attacks so dangerous—and why we’re keeping a close eye on them at AED.
xxxxxxxxxxxxxx
The Biggest Attack on Abortion Since the End of Roe
Yesterday, a federal court temporarily blocked the FDA rule that allows mifepristone to be prescribed without an in-person visit. The notoriously conservative Fifth Circuit of Appeals ruled in favor of Louisiana Attorney General Liz Murrill, who argued telehealth access to the abortion medication harms her Republican state by allowing women to sidestep its ban.
The decision is the biggest legal blow to abortion rights since the end of Roe, and conservatives hope it will end the shipping of abortion pills nationwide.
Let me be clear: that is not going to happen. Patients will continue to seek out abortion pills, and providers will continue to ship them. Nothing in this ruling criminalizes patients who use abortion medication, and women can still legally obtain abortion pills by mail—either by using a misoprostol-only regimen or connecting with a provider who will ship both medications.
That’s right: while conservatives want Americans to believe they can no longer get mifepristone by mail, multiple legal experts tell Abortion, Every Day that’s just not the case. Some providers plan to keep shipping mifepristone while the litigation plays out—relying on shield state protections that Democratic governors have put in place.
“We anticipated this moment and have worked hard with our allies at the state level to create the legal landscape and legislation to empower states to protect access to abortion nationwide,” says Julie F. Kay, founder Reproductive Futures.
To put it plainly: We are not going back.
Still, I won’t downplay the situation: this decision is a chilling attack on women’s ability to access care. With this ruling, the federal court has allowed Louisiana extremists to dictate abortion rights for the entire country—overriding laws in pro-choice states. As Reproductive Freedom for All president Mini Timmaraju put it, “The court’s decision moves us one step closer to a national abortion ban.”
Remember—telemedicine accounts for almost 30% of American abortions, and for nearly every abortion that happens in banned states. Abortion pills by mail are largely the reason the national abortion rate hasn’t dipped since the end of Roe, and telemedicine has been one of the most important tools we have holding access together.
That’s why conservatives have been hitting abortion medication so hard: they’re furious that it allows women to sidestep their draconian bans. They want to control us, and abortion pills make that much, much, harder.
I waited until now to publish for a reason: there are a lot of moving parts, things are moving quickly, and I don’t want to feed into chaos and confusion. If/When/How tells AED that their legal helpline has already been inundated with calls from patients worried that taking abortion pills is illegal. That is exactly what the anti-abortion movement wants: patients afraid, and us overwhelmed.
Since last night, I’ve been on the phone with legal experts, providers, and abortion rights leaders—and while there are different opinions about what might happen next, everyone agrees on this: what we do next needs to be steady, considered, and strategic.
And when I say “we,” I mean it. The folks who read this newsletter are activists, providers, journalists, researchers, lawyers, legislators, and organizers. Even if you don’t work in this space, chances are you’re the person a friend or neighbor comes to when they have a question about abortion. Every single one of us has a tremendous amount of influence in our own communities, and it’s vital that we’re using it wisely.
Every day that you’ve read this newsletter has prepared you for a moment like this one, and now it’s time for us to get to work.
Below is an explainer of the case, the ruling, what it means, what happens next, and what we can do. Feel free to skip around using the headers.
What is Louisiana v. FDA? - How has the Trump administration responded? - What does the federal ruling say? - Will providers really keep shipping mifepristone? - What about miso-only abortions? - How will the ruling change access to abortion? - What happens next? - How can I help?
What is Louisiana v. FDA?
Louisiana Attorney General Liz Murrill filed a lawsuit against the FDA last year, asking the court to reinstate a requirement that patients obtain mifepristone in person from their doctor. (The Biden FDA suspended that requirement during COVID, and made the change permanent in 2023.)
Murrill argues abortion pills are unsafe—citing a widely-debunked ‘study’—and claims telehealth access allows abusers to surreptitiously poison women with abortion pills. Cynically co-opting ‘coercion’ has become central to attacks on abortion medication: it allows Republicans to pretend as if they’re protecting women—which is a whole lot more popular than restricting abortion.
Murrill also says that Louisiana suffers “sovereign and financial harms” as a result of telemedicine access. This last argument is important, because the Supreme Court unanimously threw out a challenge to mifepristone in 2024, ruling that the anti-abortion doctors who brought the suit couldn’t show that they’d been personally harmed:
Murrill didn’t want the same thing happening in her case, so she claims Louisiana is being forced to spend Medicaid dollars treating women who’ve had complications from mifepristone (financial harm), and that the FDA’s rules nullify the state’s ban (sovereign harm).
It’s also important to know that this suit—and yesterday’s ruling affirming it—isn’t just about attacking abortion pills. It’s about eliminating shield laws. Republican attorneys general have been in a race to get blue state abortion protections to the Supreme Court; with this decision, the Louisiana AG is leading the charge.
How has the Trump administration responded?
We haven’t heard from the administration on yesterday’s ruling yet, but I’m betting they’re not very happy with having to deal with abortion ahead of the midterms.
That’s why Trump’s FDA asked the court to pause Murrill’s suit in January. The administration argued that the agency needed time to finish its bogus ‘safety review’ of mifepristone—but the truth is that they were desperate to delay a high-profile abortion fight until after the midterms. Republicans—Trump, especially—know this is a loser issue for them.
Still, that doesn’t mean that Trump plans to leave abortion pills alone entirely: in its request to pause the case, the administration did not disagree with Louisiana’s core argument. In fact, they even suggested the FDA could end telehealth access to mifepristone itself, depending on the outcome of its review.
In other words, they want to restrict mifepristone on their own terms and timeline. And last month, a judge gave Trump’s FDA the stay it asked for.
Yesterday’s ruling upended that plan, forcing the administration into a precarious position: either alienating the anti-abortion movement by appealing the ruling, or pissing off voters by going along with a national abortion restriction.
As law professor Mary Ziegler told The New York Times, “This ruling will put abortion back on the map as an election issue.”
What does the federal ruling say?
You can read the full decision here, but the short version is that the judges agreed with Murrill. Trump appointee Judge Kyle Duncan wrote that the FDA rules “cancel Louisiana’s ban on medical abortions and undermines its policy that ‘every unborn child is [a] human being from the moment of conception and is, therefore, a legal person.’”
The ruling temporarily pauses the 2023 FDA rules that allow mifepristone to be dispensed without an in-person visit to a medical provider.
In other words, a radical attorney general in Louisiana and Trump-appointed judges are trying to control what abortion rights look like for the entire country. So much for leaving abortion to the states!
As Sen. Patty Murray put it:
“Three judges on the most extreme appeals court in the country sided with anti-abortion politicians over the FDA's career scientists, over a quarter-century of safety data, over millions of American women who have safely used mifepristone, and over practically every major medical association in the United States.”
Will providers really keep shipping mifepristone?
Some will, yes. Telehealth abortion providers across the country are weighing their next steps right now. Providers aren’t a monolith: some will keep shipping mifepristone, while others switch to miso-only protocols while the case plays out. They’ll be making decisions based on what state they’re in, what their shield law looks like, what kinds of resources they have access to, and what their risk aversion is.
It would also help, I’m sure, if pro-choice leaders—attorneys general and governors, specifically—came out immediately to make clear that they will continue to protect providers who ship abortion pills, and that the status quo will hold while litigation continues.
AED’s legal sources point out that yesterday’s ruling is a regulatory one: it applies to the FDA, and the FDA can decide what to do next. Crucially, the agency’s enforcement authority is typically directed toward manufacturers and distributors—not providers.
“In the meantime, the people who have mife already on hand, labeled correctly and FDA compliant when they received it, could decide to continue on course until told otherwise by a federal agency,” says Rachel Rebouché, professor at University of Texas School of Law.
That’s not to downplay the risk providers have to weigh: it’s not nothing to go up against a federal ruling or the FDA—should the agency decide to go along with the Fifth Circuit’s decision. But the legal implications of shipping mifepristone in light of this ruling are not nearly as clear-cut as conservatives would like Americans to think.
What about miso-only abortions?
Even without mifepristone, you can still have a safe and effective medication abortion using just misoprostol—which was not impacted by yesterday’s ruling. Planned Parenthood has a guide to miso-only abortion here.
And while it’s important to spread the word that miso-only abortions are available, let’s be real: there’s a reason that the recommended regimen is mifepristone and misoprostol. Miso-only abortions are often longer and less comfortable. A few advocates I spoke to worried that we’d see more ER visits because of miso-only abortions—not because the regimen isn’t safe, but because patients will be in more pain.
It’s added cruelty from the anti-abortion movement.
How will the ruling change access to abortion?
Right now, two things are true at the same time: patients can still get abortion pills by mail, but this ruling is also primed to upend access to abortion and miscarriage care.
We have our work cut out for us, because we need to make sure our communities understand both. We need to thread the needle of relaying what a big deal this decision is, and how it’s a major attack on national access—but also reminding people that they can still get care, and that there are advocates across the country dedicated to helping them get it.
After years of covering this issue, I have a tremendous amount of faith that all of the worst-case scenario planning that advocates and providers have done will kick in. As Lizzy Hinkley, legal director for the Abortion Coalition for Telemedicine (ACT) says, “Shield law providers have been preparing for this moment, with support from ACT, and together we are working to ensure there are no gaps in access.”

We also know that people have already been going through informal channels to access care—like international telehealth, community networks, and websites that sell pills. This decision won’t impact those resources.
Still, let’s be clear-eyed: if the ruling stands, it will have a massive chilling effect on care. Not everyone will be able to connect with the advocates who can help them get pills by mail. Some patients will be forced to travel hundreds of miles just to pick up a prescription. Others will have to forgo abortions altogether.
What I’m most worried about? Republicans have done an unfortunately excellent job instilling fear across the country. There’s a reason states have passed laws that classify shipping abortion pills as “drug trafficking,” or have criminalized “aiding and abetting.”
That chilling effect has been made much worse by the very public moves towards criminalization more generally. American voters can see that women are being arrested for their miscarriages—why would they feel safe seeking out abortions?
No matter what happens next, the anti-abortion movement is already getting something it wants: chaos and confusion.
What happens next?
A lot will depend on what the U.S. Supreme Court and the Trump administration decide to do.
Mifepristone manufacturer Danco Laboratories has already asked SCOTUS for emergency relief, petitioning the court today to block the Fifth Circuit’s ruling. Democratic attorneys general are also expected to go directly to the Supreme Court—though it’s unclear if they’ll move quickly or wait for a response to Danco’s filing. AED sources say the AGs will seek to limit the scope of the ruling; I’ll let you know as soon as I find out.
If the Trump administration appeals, they’ll likely offer the same argument they did when asking for the stay: a defense of the FDA’s authority.
Some of my sources, however, aren’t convinced they’ll challenge the ruling at all. They think there’s a chance the administration lets it stand—giving them the opportunity to restrict abortion medication while shifting political blame onto the courts. After all, the administration is packed with Heritage Foundation maniacs—extremists not just interested in banning abortion, but birth control, IVF, and anything else that aids in women’s freedom.
And even if the administration is scared enough of abortion to hold off until after the midterms—what happens then?
Similarly, while some feel confident that the FDA’s integrity will hold through the agency’s supposed “safety study” of mifepristone, others find that idea naive.
How can I help?
Make sure your communities—online and off—know they can still legally use abortion pills. Need language for social media? I’ve got you covered:
This ruling does not make it a crime to use or seek abortion pills. If you’ve already ordered abortion pills, you’ve done nothing illegal or wrong. You can continue as planned. If you need abortion pills now, you can still get them. Go to websites like Plan C Pills or I Need An A.
Abortion, Every Day also has a robust resources page that you can share—with links to providers, legal and medical help, abortion funds, and more.
If you live in a shield state, contact your governor and attorney general.Thank them for their continued commitment to reproductive rights and women’s autonomy, tell them you don’t want Louisiana extremists dictating what happens in your state, and let them know how important it is that they protect providers who ship abortion pills across state lines.
If you live in New York, encourage Gov. Kathy Hochul to sign S8544/A9217, which further protects providers if the FDA’s approval status for mifepristone changes. (California passed a similar law last year.)
Support your local abortion fund and providers. As a result of this ruling, more patients will seek out in-person care, necessitating money for travel, lodging, child care, and the procedures themselves.
Remind people this is why elections matter. I know that can feel like a hollow thing to say when we’re watching courts dismantle rights in real time. But the anti-abortion movement has been playing a long game for fifty years—stacking courts, electing AGs, flipping state legislatures. And it’s working. We need voters to show up with the same focus and fury—especially because we have the power of the people on our side.
xxxxxxxxxxxxxx
Shield Laws for Reproductive and Gender-Affirming Health Care: A State Law Guide
After the Supreme Court overturned Roe v. Wade in June 2022 and eliminated the federal constitutional right to abortion, many states enacted bans and further restrictions on abortion. In response, states seeking to preserve and expand access to abortion have passed shield laws: legal protections for patients, health care providers, and people assisting in the provision of certain health care in states where that care is legal from the reach of states with civil, criminal, and professional consequences related to that care.
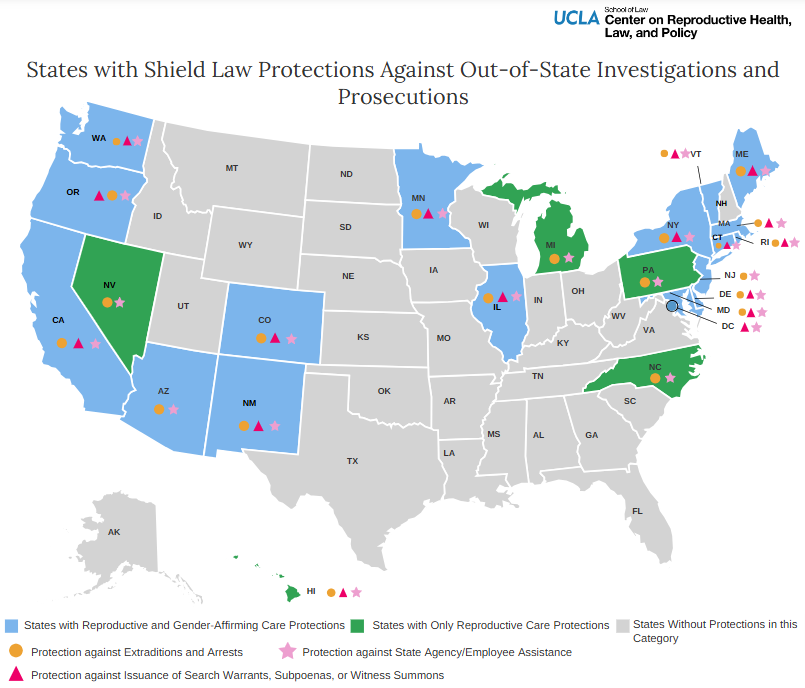
Currently, through legislation or executive order, 22 states and Washington, D.C. have shield law protections related to reproductive health care, and 18 states and Washington, D.C. have shield law protections related to gender-affirming health care. The extent and type of protections offered by each state’s shield laws vary. Legislatively-enacted shield laws in 8 states explicitly protect provision of care regardless of patient location, which includes telehealth provision.
Shield Laws for Reproductive and Gender-Affirming Health Care: A State Law Guide provides analysis of each state's shield laws. The map below shows which states have shield laws. Click on a shield law state to learn more about its specific protections for reproductive and gender-affirming health care.
The State Law Guide was last updated in March 2026.
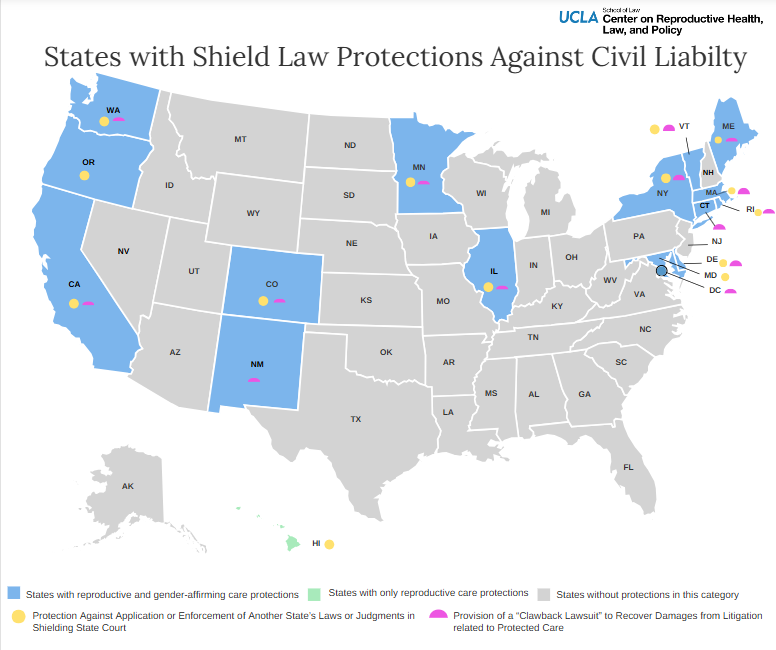
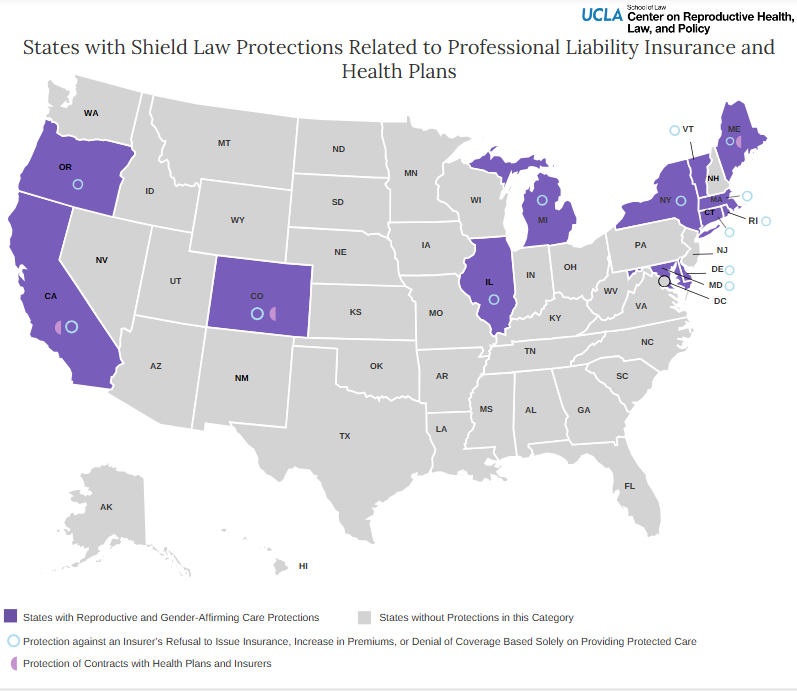
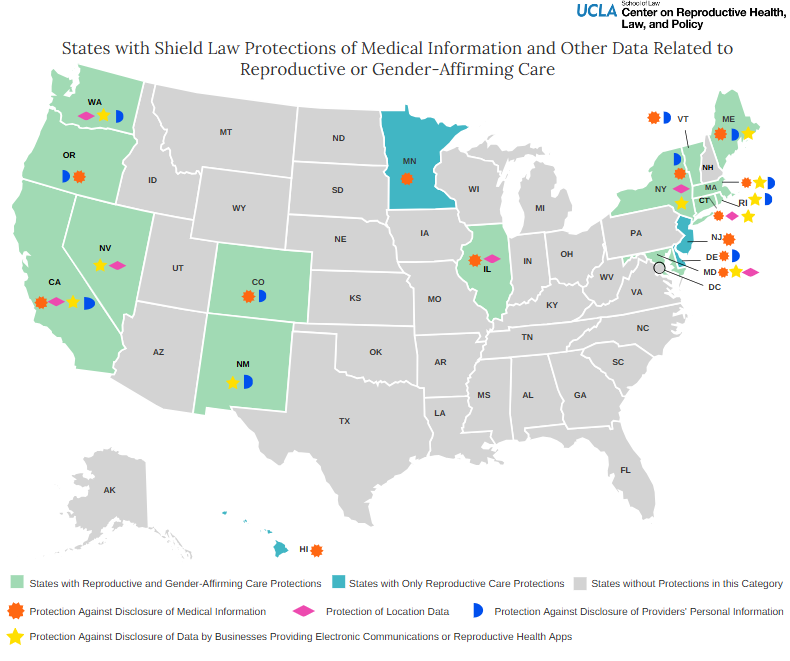
Shield Laws by Categories of Protection
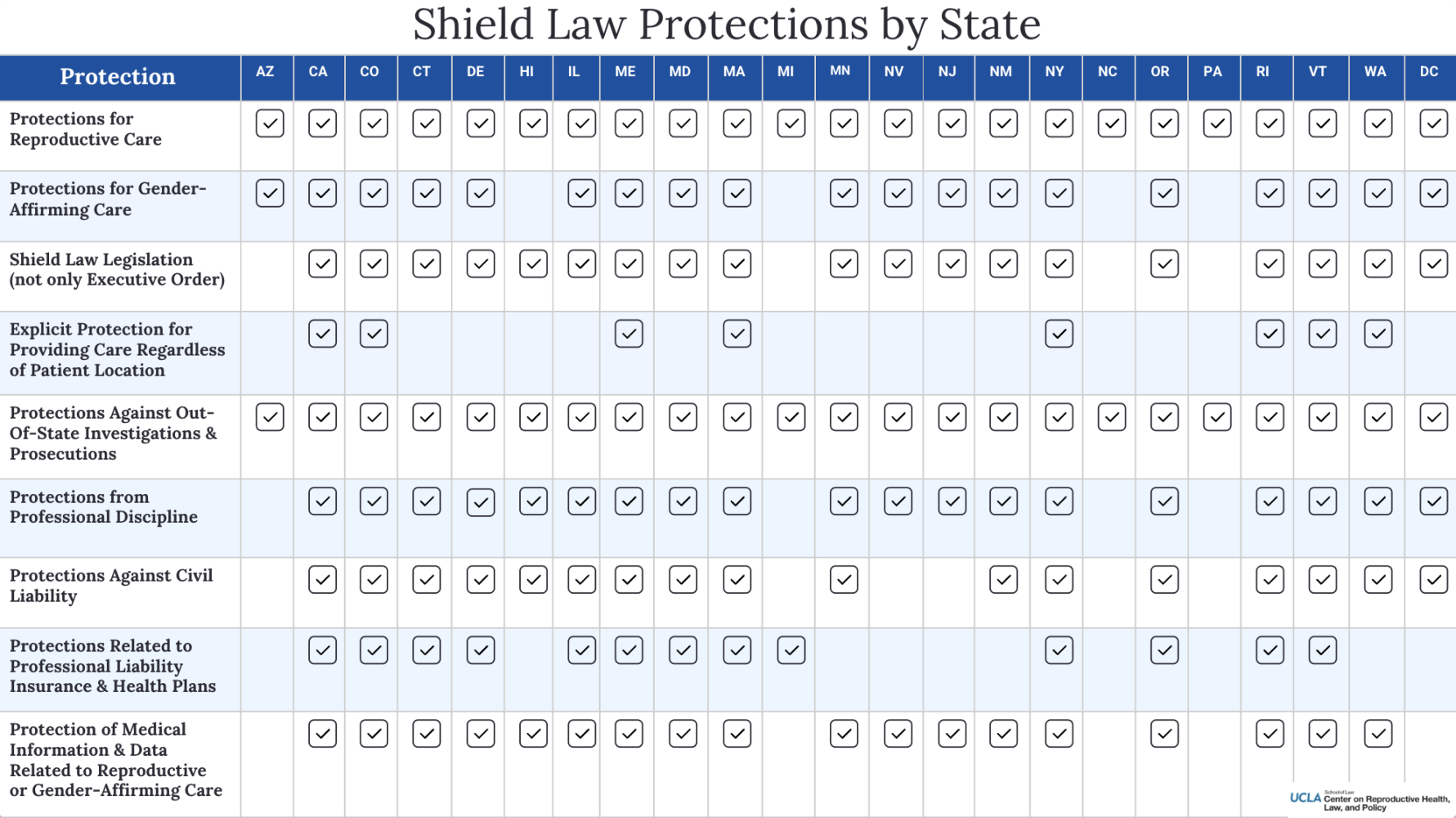
The protections offered by each state’s shield laws vary. Shield laws may include: (1) Protections Against Out-of-State Investigations and Prosecutions (including specific protections against extradition, arrests, search warrants, subpoenas, witness summons, and state agency assistance in out-of-state investigations or prosecutions), (2) Protections Against Professional Discipline (including specific protections against adverse actions related to providers’ licenses, board discipline, and denial or restriction of facility privileges), (3) Protections Against Civil Liability (including specific protections against application or enforcement of another state’s laws or judgments in the shielding state’s courts, and availability of a “clawback” action to recover damages from litigation in another state as a result of providing, receiving, or assisting in the provision of certain health care), (4) Protections Related to Professional Liability Insurance and Health Plans (including specific protections against an insurer’s refusal to issue insurance, increase in premiums, or denial of coverage based solely on providing protected care and protections for contracts with health plans and insurers), and (5) Protection of Medical Information and Other Data Related to Reproductive or Gender-Affirming Care (including specific protections against disclosure of medical information, location data, providers’ personal information, and data held by businesses providing electronic communications or reproductive health apps). 4 states only offer certain protections by executive order rather than by legislation. The legislatively-enacted shield laws in 8 states explicitly protect provision of care regardless of patient location, which includes telehealth provision.
The chart and maps below show the types of protections offered in each shield law state.
This State Law Guide is designed to provide a foundation on each state’s shield laws related to reproductive and gender-affirming health care. To receive pro bono legal assistance on questions related to the shield laws or other reproductive rights or justice issues, email larj@law.ucla.edu.
For general questions regarding the Center on Reproductive Health, Law, and Policy, email crhlp@law.ucla.edu.
xxxxxxxxxxxxxxxxxxx
The History of Mifepristone - Reproductive Health Access Project

Updated March 27, 2024
Nearly four years ago, we celebrated the 20th anniversary of mifepristone and looked back on the history of this medication and how it expanded the options available for those seeking abortion care.
French researchers developed mifepristone (also known as RU-486) in the 1980s to be taken with misoprostol for medication abortion care. Despite the outcry of anti-abortion activists, it was approved for use in France in 1988. In the United States, however, it was a very different story, as the FDA banned the importation of mifepristone in 1989. The manufacturer of mifepristone, Roussel-Uclaf, also banned mifepristone distribution in the United States and refused to supply it to researchers investigating the drug’s other possible health benefits.
The first challenge of this ban in the courts was by an American woman named Leona Benten, who was stopped by US Customs when bringing mifepristone into the country from the United Kingdom. Although Benten lost her case, it brought mifepristone into the national spotlight and galvanized the movement to overturn the FDA ban. When President Bill Clinton was elected in 1993, he ordered the Department of Health and Human Services to investigate mifepristone’s use for medication abortion. In 1995, Roussel-Uclaf agreed to give the Population Council the patent rights to mifepristone in the United States.
Although the FDA’s advisory branch recommended mifepristone for approval, legal and manufacturing troubles led to the medication being pushed to the side until 2000. Thanks to the work of activists and health professionals, mifepristone was finally approved for medication abortion on September 28, 2000, twelve years after its original synthesis.
Today in the US, medication abortion with mifepristone and misoprostol is provided in-clinic and via telehealth up to 11 weeks gestation. In 2023, medication abortion accounted for 63% of all US abortions, up from 39% in 2017 and 53% in 2020. Medication abortion has only been growing, especially as access to self-managed medication abortion information and support has increased due to the needs and preferences of communities most impacted by barriers to healthcare, abortion bans, and restrictions.
Unfortunately, mifepristone remains inaccessible to many people. The US Food and Drug Administration (FDA) regulates mifepristone under a Risk Evaluation and Mitigation Strategy (REMS), which means it’s classified as a “dangerous drug” – despite its history of safe and effective use. There is an overwhelming body of scientific and medical evidence that shows mifepristone is safe and effective for virtually anyone in a variety of practice settings, including telehealth, in-clinic, and self-managed care. Until recently, the REMS rules on mifepristone required them to stock and dispense the pill directly to patients in-office, creating barriers to providing mifepristone in primary care settings. When mifepristone is inaccessible in primary care, patients are harmed. Their continuity of care is disrupted, emotional and financial consequences are exacerbated, they experience unnecessary and invasive procedures, and they must manage multiple appointments and delays in care.
Early in the ongoing global COVID-19 pandemic, the REMS rule required patients to travel to the clinic to pick up mifepristone in-person, forcing those seeking abortion care to risk needless exposure to the virus. The FDA had allowed patients to obtain nearly all other REMS-classified drugs by mail to avoid COVID-19 risks, but mifepristone was still required to be picked up at a clinic, even though it can be taken later at home. In the spring of 2020, the American Civil Liberties Union (ACLU) filed a lawsuit on behalf of a coalition of medical experts and reproductive justice advocates to fight this rule. On July 13, 2020, a federal district court issued a preliminary injunction that blocked the FDA from enforcing its in-person pick-up requirement for medication abortion until at least 30 days after the end of the federal government’s declared public health emergency. This ruling was particularly important for low-income communities and those who are Black, Indigenous, and People of Color, as they make up the majority of those disproportionately impacted by COVID-19.
The preliminary injunction became an official REMS modification in January 2023, allowing clinicians to not only mail mifepristone to their patients but also to prescribe the pill to certified pharmacies for patients to pick up or receive by mail. However, barriers still remain. For states that already outlaw telemedicine for medication abortion or ban abortion entirely, these rules do not apply.
Today, there are threats to nationwide access to mifepristone through the Alliance for Hippocratic Medicine v. Food and Drug Administration case. Which is trying to force the FDA to remove mifepristone’s approval. This is entirely based on politics, not on medicine, science, or law. It is an extension of our nation’s history and the ongoing presence of reproductive coercion and control.
In oral arguments on March 26th, we were encouraged to hear the Justices’ skepticism that these anti-abortion groups have standing to pursue this baseless case. In reality, this case should have never gotten this far.
This case is part of an agenda to ban medication abortion – and all abortion – across the country. It attempts to prevent people from accessing abortion medication with threats of investigation, jail, and prosecution. If you are concerned about the abortion laws in your state, including self-managed abortion and the law, If/When/How’s Repro Legal Helpline provides free legal information and advice at reprolegalhelpline.org or 844-868-2812. And, if you need legal advice or representation for providing or helping others access abortion care, contact the Abortion Defense Network.v
xxxxxxxxxxxxxxxxxxxxx
The group suing the FDA over its abortion pill approval claimed that 1 in 5 women will suffer a complication from medication abortion. The figure appears to come from a 2009 study that experts say is flawed. Even its lead author said the claim distorts the research.
After two judges, one in Texas, the other in Washington, issued dueling rulings on access to the abortion pill mifepristone, it stirred social media discussion about the medication’s safety.
A Facebook video shared in March by Alliance Defending Freedom, the Christian legal group representing anti-abortion groups and doctors in the Texas lawsuit, received renewed attention and thousands of views.
"This case is about protecting women and girls from the dangers of chemical abortion drugs,"Alliance Defending Freedom attorney Erica Steinmiller-Perdomo said in the March 27 video. "The fact is these drugs are dangerous — 1 in 5 women will suffer a complication."
Medication abortion, which involves a combination of two medicines — mifepristone and misoprostol — typically taken around 24 hours apart, accounts for more than half of all U.S. abortions and has been used by more than 5 million women, according to the Guttmacher Institute, an abortion-rights research organization. It has become the only method available to many women living in states where abortion has been banned.
The U.S. Food and Drug Administration has repeatedly reaffirmed mifepristone’s safety since it was first approved in 2000. (Misoprostol has been on the market longer and has different uses, including preventing stomach ulcers).
PolitiFact reached out to Alliance Defending Freedom for evidence supporting its "1 in 5" claim. We did not receive a response by publication. But the alliance’s lawsuit cites a 2009 study from Finland.
We found the same statistic on the website for the anti-abortion Charlotte Lozier Institute, which also cited the Finland-based research. That study evaluated national registries for women in the country who had abortions between 2000 and 2006 and found that about 20% who took medication abortion said they experienced adverse events.
The study’s lead author said the claim distorts her research, and experts told us the research is flawed. The paper didn't use a standardized definition for adverse events. It included cases where women took mifepristone alone or misoprostol with another drug. And it included complications that required no medical intervention.
In a comprehensive analysis of research on the topic, The New York Times showed that more than 100 studies reviewing 124,000 abortions over 30 years have found medication abortion to be safe and effective for women.
"I think (mifepristone) is one of the best studied medications that’s currently on the market," Dr. Daniel Grossman, a professor of obstetrics, gynecology and reproductive sciences at the University of California, San Francisco, told PolitiFact. "There’s been a lot of research done on this treatment, and study after study shows that medication abortions are very safe and very effective."
One day, two competing mifepristone rulings
On April 7, U.S. District Judge Matthew Kacsmaryk, an appointee of former President Donald Trump, ruled in Texas that the FDA lacked the authority to approve mifepristone more than two decades before. The decision would suspend the agency’s approval, which could trigger its removal from the market. Kacsmaryk wrote that his decision would go into effect after seven days, giving the Justice Department time to appeal.
That same day in Washington state, U.S. District Judge Thomas Rice, whom former President Barack Obama appointed, found the opposite in a separate case, and issued an order prohibiting the FDA from pulling access to mifepristone in 17 Democratic-led states that sued over the issue.
The rival rulings add legal confusion to a growing tangle of abortion-litigation across the country following the Supreme Court’s June 24, 2022, decision to overturn Roe v. Wade.
On April 10, the federal government asked the 5th Circuit Court of Appeals to block the Texas order pending its appeal. The court ruled April 12 that mifepristone could remain available, but imposed temporary restrictions that rolled back more recent changes the FDA made to improve access to the drug, including patients getting the pills by mail.
More than 400 drug company leaders — none of which make mifepristone — condemned the Texas ruling in a signed statement that said the decision ignored decades of scientific evidence and legal precedent and called for its reversal.
"If courts can overturn drug approvals without regard for science or evidence, or for the complexity required to fully vet the safety and efficacy of new drugs, any medicine is at risk for the same outcome as mifepristone," the statement said.
In an April 8 post announcing its appeal of Kacsmaryk’s decision, the FDA said it "stands behind its determination" that mifepristone is safe and effective under its approved conditions of use for medication abortion, and added that patients should have access to FDA-approved medications.
The source of the ‘1-in-5’ complications claim
In 2009, researchers in Finland published a paper in the Obstetrics & Gynecology medical journal. The study consulted three of the country’s national health registries for 42,619 women who, from 2000 to 2006, had abortions through their eighth week of pregnancy. The patients were followed until about six weeks following their abortions.
About 22,000 had medication abortions; the other 20,000 underwent surgical abortions. Researchers reported that about 20% of the women who took medication for their abortions experienced what the paper described as adverse events or complications, with hemorrhage making up the lion’s share at 15.6%
But experts said there’s a glaring issue with hemorrhages it classified as "complications." These situations were defined in the study as excessive bleeding that involved clinician consultation, and the paper doesn’t say whether they required medical interventions or blood transfusions.
"We know that bleeding is an expected outcome with medication abortion and people are told about it in advance," Grossman said. "But this study doesn’t have a standardized definition of hemorrhage, and there was no reporting on transfusions."
Maarit Niinimäki, the study’s lead researcher and consultant gynecologist at the University Hospital of Oulu, Finland, also told PolitiFact in an email that the 1-in-5 claim distorts her research.
"We concluded that medical abortion is generally safe and serious adverse events were rare," Niinimäki said. "As this was a register-based study, we reported all visits in the hospital for various indications, many of them were for benign reasons and did not lead to intervention."
Niinimäki also said bleeding is a result of the abortion process and isn’t dangerous in the majority of cases.
"Sometimes a patient comes to a check-up visit if she’s worried. But you can not get detailed information of the visits when having a register-based study," Niinimäki said.
Niinimäki said that when her study was published, medication abortion was a new method in Finland and the routine for follow-up was not well established and likely caused additional visits.
"We are independent researchers aiming to publish the results honestly without (a) political agenda, and we never claimed that medical abortion with mifepristone/misoprostol protocol is a dangerous procedure and should be abandoned," Niinimäki said.
Critique of the Finland study
Grossman called the Finland study "very nonspecific" because it’s based on coding that providers entered following their clinical encounters.
Ushma Upadhyay, a professor and public health scientist at University of California, San Francisco and lead author of a 2015 study on emergency department visits and complications after abortion, said the Finland study "is simply not rigorous."
"It didn’t use standard definitions of adverse events, and the most notable weakness is its classification of hemorrhage without additional treatment," Upadhyay wrote in an email.
"The fact that these patients simply consulted with their clinician, but were not deemed to need additional treatments suggests that these were not adverse events," Upadhyay said. "They had bleeding, that is part of the expected effects."
The paper’s authors acknowledged this in their report, writing that "because medical abortion is associated with uterine bleeding lasting approximately 2 weeks, the high rate of consultation is not surprising."
Experts also noted that the study suggested that some women received mifepristone alone, which is known to be associated with increased adverse events, they said.
More than 100 studies have found abortion medication to be safe
The more than 100 studies on the abortion pills concluding that the medication regimen is safe found that the rate of major complications requiring treatment, such as severe hemorrhages or infection, is very low.
Upadhyay’s study, which assessed around 11,000 medication abortion cases, found that these types of complications amount to about one-third of a percent.
Upadhyay said that anti-abortion activists have misrepresented her data about emergency department visits to try to support their claims that abortion is unsafe. (Her study is referenced on the same Charlotte Lozier Institute webpage as the Finnish study.)
But these visits do not signal complications, she said, and research has shown that patients who live farther away from where they received an abortion were more likely to go to the emergency room for reassurance or to confirm that the abortion was successful. Another study found that around 51% of abortion-related emergency department visits involve observational care only, with no diagnosis or treatment.
"This really shows that people go to the emergency department to have their questions answered. They aren’t getting any treatment. They are being observed and released," Upadhyay said. "They don’t have a nearby abortion provider for help, so they’re going to go to the closest safety net provider that they can that’s open 24/7."
Mifepristone is considered safer than many common drugs, including Tylenol and Viagra, and when used in the recommended protocol with misoprostol, successfully terminates pregnancy 99.6% of the time, with a 0.4% risk of major complications, the Kaiser Family Foundation reported.
The FDA’s latest data is comparable, with five deaths associated with mifepristone for every 1 million people in the U.S. who have used the drug since its approval in 2000. That’s a mortality rate of 0.0005%.
Our ruling
A video from Alliance Defending Freedom claimed abortion pills are dangerous and that "1 in 5 women will have a complication."
The statistic appears to be based on a flawed study that experts said misclassified complications. The study’s lead author said the claim misconstrues the research. More than 100 studies spanning multiple decades have found that medication abortion is safe and effective.
We rate this claim False.
xxxxxxxx
Abortion pills by mail surge despite Texas' bans. Will it last?

Nurse practitioner Debra Lynch, founder of Delaware-based Her Safe Harbor, writes a note Dec. 5, 2024, to go into a medication abortion package that will be mailed to a patient. "I might be the only person that's speaking to them about this, that actually knows what they're going through," she said. "I'm just trying to let them know that I am here for them."
Bridget Grumet/American-StatesmanNEWARK, DELAWARE — The large cardboard box in Debra Lynch’s living room contained enough pills for 162 medication abortions. Last summer, such a shipment would last a month. Then she needed to reorder every two weeks. Now she goes through a box like this every week.
“We’re mailing a lot to Texas,” said Jay Lynch, who handles most of the packaging and postage for Her Safe Harbor, an abortion-drug-by-mail service spearheaded by his wife.
Advertisement
Article continues below this ad
Debra Lynch, a nurse practitioner, prescribes the pills via telehealth under Delaware law. Her husband drops the medications into white, bubble-padded envelopes that will cross state lines and defy state bans to reach the hands of anxious women.

Debra Lynch, a nurse practitioner and founder of Her Safe Harbor, unboxes a shipment of abortion medications on Dec. 5, 2024, in the living room of her Delaware home. Operating under Delaware's shield law, Lynch prescribes abortion medications via telehealth, largely to patients in abortion-restricted states like Texas.
Bridget Grumet/American-Statesman




From the kitchen table in the couple’s split-level suburban home, Jay Lynch thumbed through the shipping labels for the next two dozen orders: Alabama. Indiana. Georgia. Several in Florida. And plenty in Texas: Tomball. Houston. Beaumont. Fulshear.
“Everybody – Aid Access, ourselves, some of these other small groups – we are all shipping to Texas,” Debra Lynch said. The orders kept coming in – “I just got one from El Paso,” Jay Lynch told me later that afternoon, after his laptop and cellphone chimed – underscoring the inescapable fact that Texas’ bans have not erased Texans’ demand for abortion.
Advertisement
Article continues below this ad
Scores of telehealth abortion providers have cropped up since the U.S. Supreme Court’s Dobbs decision in 2022 allowed states to prohibit the procedure. Some telehealth providers serve patients only in states that allow abortion. But some – including major players Aid Access and the Massachusetts Medication Abortion Access Project, as well as smaller startups like Her Safe Harbor – are designed to serve patients anywhere.
In short order, these providers have had a seismic impact. Not long ago, in April 2022, about 1 in 25 abortions in America were from pills prescribed via telehealth. By June 2024, it was 1 in 5, according to the latest #WeCount report from the Society of Family Planning.
Nearly half of those prescriptions went to patients in states with abortion bans or restrictions on telehealth abortion.
Advertisement
Article continues below this ad

A shipment containing enough pills for 162 medication abortions is unpacked Dec. 5, 2024, at Delaware-based Her Safe Harbor. The telehealth provider goes through a shipment of this size every week.
Bridget Grumet/American-StatesmanTexas has outlawed most abortions (providers risk up to 99 years in prison and at least $100,000 in fines) and forbids sending abortion medication through the mail. That didn’t stop about 2,800 Texans per month from receiving abortion medication by mail in the first half of 2024 – more than any other abortion-restricted state, according to #WeCount data. (Notably, Texas criminalizes only the act of sending the pills, not receiving them.)
Looking at the national picture, more than 1 million Americans terminated pregnancies in 2023 – the highest number in more than a decade – despite the fact that 12 states have outlawed abortion and four others ban the procedure after six weeks, before many people know they’re pregnant. About 170,000 Americans (including more than 34,000 Texans) flew or drove across state lines in 2023 to get an abortion, according to the Guttmacher Institute, which supports access to abortion. But many others ended their pregnancies with pills that came in the mail.
Some are even buying pills preemptively, just in case they're needed later.
Advertisement
Article continues below this ad

From the living room of his Delaware home, Jay Lynch assembles 22 medication abortion packages on Dec. 5, 2024 for Her Safe Harbor. His wife, nurse practitioner Debra Lynch, founded the telehealth service to reach patients in abortion-restricted states.
Bridget Grumet/American-StatesmanAll of which makes these pills a central target for those who oppose abortion. Texas lawmakers and members of the incoming Trump administration could try to curb access, and Texas Attorney General Ken Paxton has been escalating the fight. A week after I visited Her Safe Harbor’s Delaware operations in early December, Paxton sued a similar provider in New York.
“In Texas, we treasure the health and lives of mothers and babies, and this is why out-of-state doctors may not illegally and dangerously prescribe abortion-inducing drugs to Texas residents,” Paxton said in a statement then.
When I caught up by phone with Debra Lynch, she was unsurprised and undeterred. “I don't fear Ken Paxton,” she said. “I don't fear getting arrested or anything like that.”
Advertisement
Article continues below this ad
What scares her the most is the possibility that Texas women “might do something dangerous to themselves because they feel desperate and isolated,” she said. “I want women to know that there are people out there working to help them.”
Two events supercharged telehealth abortion
Debra Lynch’s nursing career led her to hospitals, hospice care, homebound patients and even the subway tunnels of Philadelphia, where she offered checkups and COVID-19 vaccinations to people experiencing homelessness. By the time Lynch grew worried about another set of patients cut off from care – those living under abortion bans – two events made it possible for her and other organizations to reach across state lines to help.
Advertisement
Article continues below this ad
First, the pandemic prompted the U.S. Food and Drug Administration to drop the requirement for an in-person visit for patients to obtain mifepristone, the first pill in the medication abortion regimen for patients up to 10 weeks into a pregnancy. (Patients take the second medication, misoprostol, on their own 24 to 48 hours later.)
Then in 2022, as the Dobbs decision came down, some states started passing “shield laws” to protect medical providers in their communities from investigations or lawsuits if they provided abortions to patients from other states. Now, 23 states and the District of Columbia have shield laws of varying degrees.

Alexandrea Lopez holds up stickers to passers-by while chanting with other abortion rights demonstrators along Guadalupe Street in Austin, on Dec. 1, 2022. The protest was held on the one-year anniversary of the U.S. Supreme Court hearing arguments in the case that would eventually overturn Roe V. Wade.
SARA DIGGINS/AMERICAN-STATESMANNew York’s shield law, for instance, prohibits its agencies from cooperating with an out-of-state investigation, honoring subpoenas or extraditing defendants.
Advertisement
Article continues below this ad
That makes it “virtually impossible for a prosecutor or civil attorney” to build a case against an out-of-state doctor, according to the anti-abortion Charlotte Lozier Institute, which says shield laws enable "pro-abortion states" to "force abortion on life-affirming states."
Aid Access, which got its start serving U.S. patients from overseas, moved into five shield law states in June 2023. The Massachusetts Medication Abortion Access Project, led by Cambridge Reproductive Health Consultants president and co-founder Dr. Angel Foster, launched a few months later.
“We're now serving about 2,500 patients a month,” Foster said of her program, better known as the MAP. “About a third of those patients are from Texas, and 95% of our patients are from states where there are abortion bans, restrictions or bans on telemedicine.”
Illustrating the impact of this effort, Foster pointed to Mississippi, which had about 3,600 abortions a year before the Dobbs case shuttered the state’s last abortion clinic.
Advertisement
Article continues below this ad
Now, with the combined efforts of Aid Access and the MAP, “we’ll probably provide care to over 4,500 patients in Mississippi in 2024,” she said. And that care is more affordable, too: The MAP uses a pay-what-you-can model starting at $5, and Aid Access charges up to $150, while clinic-based medication abortions typically cost more than $500.

Jay Lynch holds a sealed bottle of misoprostol, the second set of pills used in a medication abortion regimen. Numerous telehealth providers, including Delaware-based Her Safe Harbor, send abortion medications to patients in abortion-restricted states like Texas.
Bridget Grumet/American-StatesmanThat’s not to minimize the harm inflicted by abortion bans, including the fact that some patients still can’t access care, Foster said.
“But it is easier and cheaper to get a medication abortion in Mississippi today than it was four years ago,” she said, “and I think that is a pretty incredible thing that's happened because of the shield laws in the post-Dobbs environment.”
Advertisement
Article continues below this ad
Both sides planning countermoves
Joe Pojman, the founder and executive director of the Texas Alliance for Life, is also astonished by the rise of telehealth abortion – for entirely different reasons.
“It makes no sense that any responsible doctor would send pills to a woman out of state without ever examining that person personally, and without having a license to practice medicine in Texas,” said Pojman, who also asserted that medication abortion is dangerous, despite more than 100 studies finding it to be safe and effective. “If it were happening in any other specialty of medicine, I think people would be outraged.”
He applauded Paxton’s lawsuit against the New York doctor, hoping the courts will strike down the shield laws. But no one is confidently placing bets.
Advertisement
Article continues below this ad
When I asked abortion law expert Mary Ziegler, a professor at the University of California at Davis School of Law, whether shield laws are likely to withstand judicial scrutiny, she replied, “I think the short answer is ‘who knows,’ combined with a fair amount of ‘it depends.’”

The Austin Women’s Health Center is one of many former abortion clinics struggling to keep its doors open since the Dobbs decision, but they continue to give women other forms of reproductive health care: providing birth control, managing miscarriages and testing for sexually transmitted infections. Many Texans seeking abortion care have to turn to out-of-state telehealth providers.
Jay Janner / American-StatesmanIn the meantime, Texas lawmakers are looking to fortify the state’s abortion bans. One proposal, House Bill 991 by Rep. Steve Toth, R-The Woodlands, aims to cut off access to medication abortion by empowering private citizens to sue internet service providers who fail to block such websites in Texas.
Plan C, one of the websites singled out by name in HB 991, provides state-by-state information and links to places people can obtain pills. Plan C co-founder and co-director Elisa Wells said the site typically receives about 5,000 to 6,000 visitors a week from Texas. That number shot up to 23,000 the week that Donald Trump won the presidential election.
Advertisement
Article continues below this ad
“I think everybody is planning for the worst,” Wells told me. “I mean, you have to assume that what's written in the Project 2025 plan is something that will be a road map for the Trump administration.”
The plan, written by the Heritage Foundation and other conservative groups, calls for immediately reinstating the requirement that mifepristone be dispensed in person, essentially outlawing telehealth abortion; and ultimately revoking the FDA's approval of mifepristone, which would take that drug off the market entirely (something the U.S. Supreme Court declined to do in 2024).
Project 2025 also argues the feds should reanimate the Comstock Act – a long-dormant anti-obscenity law from 1873 – to prosecute anyone who sends abortion-related items through the mail.
Asked last month on "Meet the Press" whether his administration would restrict the availability of abortion pills, Trump said, “The answer is no.” But he refused to make a firm commitment, noting “things change.”
Advertisement
Article continues below this ad
Wells said if the feds crack down on the mailing of abortion pills, “there are alternate routes of access that we know about that we've been researching for the last 10 years, that we believe will still be operational.”
They’re already listed on the Plan C website: Telehealth providers based outside the U.S.; websites that sell pills without providing medical support; and volunteer-run community support networks that provide pills for free.
Under Texas law, patients cannot be charged for seeking or obtaining an abortion. The bans target providers. Still, there are legal risks. Anyone helping a patient – say, a partner or relative paying for the pills – could be sued in Texas for abetting an abortion. And in rare cases, authorities overreach: Starr County prosecutors in 2022 charged a South Texas woman with murder for a self-induced abortion, subjecting her to public humiliation before the charges were dropped three days later.
“But at the end of the day, there is just this absolutely relentless network of activists and organizations all over the country who are dedicated to helping people access abortion, no matter what the law says,” said Amelia Bonow, founder of the advocacy group Shout Your Abortion. “And that's not going anywhere.”
Advertisement
Article continues below this ad
'There's almost a pleading in their voice'
From the kitchen table headquarters of Her Safe Harbor in Delaware, Debra Lynch told me she planned to order as many pills as she could before Trump takes office. If the landscape changes and she needs to move outside the country to continue this work, she said, she will.
“No matter what obstacle might come down, we're trying to think ahead and make sure that we can figure out another way around it,” said Lynch, who has more than a dozen volunteers helping with Her Safe Harbor. “Because the ultimate goal is to make sure the medication is available to the women who need it.”
It was time for Lynch to call a young woman who had sent a worried message through the website. The patient had finished the second step of the abortion medications four days ago and was still cramping and bleeding heavily. Is this normal? the patient wondered.
Advertisement
Article continues below this ad
Lynch asked detailed questions of the woman, who agreed that I could listen to the call. I didn’t know her name or location. Her soft replies of “yes, ma’am” suggested somewhere South.
Lynch finally told the patient to rehydrate with a drink packed with electrolytes and then plan on taking another dose of misoprostol in a few hours.
“Would you be OK if I did a check-in call with you tonight?” Lynch asked.
“Yes,” the woman said, relieved that she wasn't on her own. “That would be great.”
Advertisement
Article continues below this ad

Nurse practitioner Debra Lynch holds one of the personalized notes she wrote Dec. 6, 2024, to a patient who will receive an abortion medication packet. "It lets them know that there's a person on the other end," said Lynch, founder of the Delaware-based telehealth provider Her Safe Harbor, which primarily serves patients in abortion-restricted states.
Bridget Grumet/American-StatesmanWhen they hung up, Lynch turned to me. She has two daughters, now in their 20s. She hears their voices, scared and alone, on these patient calls.
“You can hear them trying to steel themselves and not let their voice shake,” Lynch said. “But then there's also almost a pleading in their voice, like, ‘Please tell me whatever you can to make me feel cared for, that somebody is going to make sure I'm OK.’”
She stewed over the emptiness of the abortion bans. They hadn’t stopped her from mailing the medications. They hadn’t stopped patients from receiving them. They just created hundreds of miles between patients and providers. They left women feeling isolated and afraid to access a procedure that’s legal in half the country, and which had been legal everywhere in the U.S. for half a century.
Advertisement
Article continues below this ad
“They’re truly alone. That frightens the hell out of me,” Lynch said. “The mom in me, the grandma in me, wants to reach through the phone and hold these girls during all of this.”
The patient reached out again two hours later, saying her cramping and bleeding had “lessened immensely” after she rehydrated. Lynch told her the additional misoprostol wouldn’t be needed. The woman’s uterus had finished contracting on its own.
Lynch still urged the patient to get checked out for a possible respiratory infection, as the woman had mentioned having difficulty taking deep breaths.
“Do you know where you plan on going to get that (chest) X-ray?” Lynch asked.
Advertisement
Article continues below this ad
“I’ll probably just do it at my local Baylor Scott & White,” the woman said.
The hospital chain serves Central and North Texas.
By the numbers:
Advertisement
Article continues below this ad
- 4,700: Abortions provided in Texas per month in 2019, before any bans
- 5: Abortions provided in Texas per month, on average, in 2023, once state laws allowed the procedure only to protect the mother's life
- 2,850: Texans traveling out-of-state each month for abortions in the second half of 2023
- 2,800: Telehealth abortions obtained each month by Texans in the first half of 2024
- Sources: Texas Health and Human Services; Guttmacher Institute; #WeCount report
- xxxxxxxxxxxxxxxxxxxxxx
New Gov't Website Will Help CPCs Collect Data On Pregnant Women
Click to skip ahead: Moms.gov Will Help CPCs Collect Data On Pregnant Women; SCOTUS Pushes Mifepristone Decision Until Thursday; Is Trump Firing FDA Chief Marty Makary?; Legislation Watch: Abortion Pill ‘Trafficking’;In the States: Montana, South Carolina, Massachusetts, Texas & More; AED in the News; Mifepristone Attacks 101
Moms.gov Helps CPCs Collect Data On Pregnant Women
The Trump administration is encouraging pregnant women to visit Moms.gov, a new government website that directs users to a Heartbeat International data collection tool. And yes, it’s exactly what it sounds like.
This new government website—first reported by Mother Jones—is not just about sending women to crisis pregnancy centers. Moms.gov funnels vulnerable women to Option Line, one of the tools that Heartbeat International uses to collect massive amounts of data on pregnant women.
Privacy International flagged Option Line’s sketchy practices back in 2019, as did Senate Democrats in 2022—pointing out that Heartbeat International had already used Option Line to collect information from millions of American women. Last year, Kylie reported that Option Line’s terms of use allow anti-abortion activists to use any information submitted through the site “for any and all purposes… appropriate to the mission and vision of Option Line.” And Abortion, Every Day found that Heartbeat shared women’s personal medical information with corporate employees, CPC volunteers, and—in one case—anyone with an internet connection.
We’re talking about names, addresses, marital status, menstruation dates—deeply personal information. Absolute nightmare shit.
Still, the launch of Moms.gov shouldn’t come as a surprise: back in 2023, I broke the news that Republicans had introduced legislation to launch a government-run website that would direct pregnant women to CPCs while collecting their personal information. They wanted to call it “life.gov.” In 2024, conservative legislators led by U.S. Sen. Katie Britt introduced a near-identical bill. This time, though, they tried to be less obvious: they switched “life.gov” to “pregnancy.gov.”
So it’s not exactly shocking that Britt stood behind Donald Trump yesterday as he announced the launch of this latest iteration. Moms.gov is the culmination of years of work by conservative lawmakers—who are eager to partner with anti-abortion powerhouses like Heartbeat International under the guise of helping pregnant women.
I’ll have more on Moms.gov tomorrow, including the site’s MAHA-coded messaging around “preconception health” and so-called “fertility awareness-based methods.” 🫠
SCOTUS Pushes Mifepristone Decision Until Thursday
The U.S. Supreme Court has pushed off a decision on mifepristone until Thursday, meaning the abortion medication will remain fully accessible by mail for at least the next few days.
A refresher: A little over a week ago, a federal court temporarily blocked the FDA rule allowing mifepristone to be prescribed without an in-person visit. The notoriously conservative Fifth Circuit Court of Appeals ruled in favor of Louisiana Attorney General Liz Murrill, who argues that telehealth access to the abortion medication harms her Republican-led state by allowing women to sidestep its ban.
While some abortion providers immediately switched to shipping only misoprostol—the second of the two medications used to end a pregnancy—others continued sending both mifepristone and misoprostol. (Read Abortion, Every Day’s explainer to understand why.)
A few days later, SCOTUS paused the Fifth Circuit ruling to give the parties time to file additional arguments. That pause was set to expire today. By extending it for a few more days, SCOTUS is giving itself more time to decide what to do next.
So what could happen on Thursday? The justices could:
Extend the stay again, pushing back a decision even further;
Send the case back to the lower court and ask the Fifth Circuit to reconsider a specific issue;
Agree to take up the case on the merits, potentially on an expedited timeline;
Or rule that Louisiana lacks standing to bring the suit at all.
Murrill has worked hard to avoid that last outcome—because it’s exactly what killed the last mifepristone case before SCOTUS. In that case, the justices unanimously ruled that the anti-abortion doctors and organizations behind the lawsuit lacked standing to challenge the FDA’s regulations on the abortion medication.
In the meantime, the Trump administration has said absolutely nothing about the federal court ruling, the Supreme Court pause—any of it. It’s almost as if they know this is a loser issue for Republicans.
Is Trump Firing FDA Chief Marty Makary?
After a months-long campaign to oust FDA Commissioner Marty Makary, the anti-abortion movement may finally be getting what it wants: multiple outlets reported Friday that Donald Trump plans to fire Makary. The news broke just hours after anti-abortion leaders—including Marjorie Dannenfelser of Susan B. Anthony Pro-Life America—met with White House officials to complain that the FDA chief hasn’t been aggressive enough on abortion pills.
Here’s where things get murky: when Trump was asked directly about reports that he signed off on firing Makary, he responded, “I’ve been reading about it, but I know nothing about it.” So now we play the waiting game.
As you probably remember, Makary promised late last year that the FDA would conduct a “safety review” of mifepristone—but the administration has been slow-walking the process ever since. That’s because Republicans understand just how unpopular abortion restrictions are, and the Trump administration clearly doesn’t want a massive public fight over abortion pills heading into the midterms. (So much for that!)
I’ll keep you updated as we learn more—but if Trump does move forward with firing Makary, no one should expect his replacement to be any better.
Legislation Watch: Abortion Pill ‘Trafficking’
I’m sorry to tell you that Oklahoma Gov. Kevin Stitt has signed legislation making the ‘trafficking’ of abortion pills a felony punishable by up to ten years in prison. Under HB 1168, it’s not only a crime to deliver abortion medication, but to possess the pills with the intent to deliver them.
This language around “intent” is not an accident. The goal isn’t just to target abortion pills, but the infrastructure that makes it possible for women to get abortion medication in spite of state bans. After all, abortion pills being shipped into the banned states is a huge reason the national abortion rate hasn’t budged. Republicans know that, and it’s why they want abortion funds, activists—even those supporting a friend or family member—to be too afraid to help.
As AED has noted before, this kind of legislation also raises broad questions about what exactly counts as “delivery” or “intent.” Is a volunteer who connects women to out-of-state providers “delivering” abortion pills? What about a website that links to providers?
And Oklahoma isn’t alone here. It wasn’t so long ago that Mississippi’s governor signed a similar law that criminalizes “intent” to deliver abortion pills. (Both bills, Students for Life says, were based on their model legislation.)
The good news? As law professor Mary Ziegler has pointed out before, “intent” is very difficult to prove. Another advocate I spoke to called it “loser” legislation. But even weak laws can do real damage. The point here is the chilling effect.
Nimra Chowdhry, senior state legislative counsel at the Center for Reproductive Rights, called the law “a disgusting attempt to scare Oklahomans out of seeking abortion care and scare parents, friends, and doctors away from helping them.”
And while bill sponsor Sen. David Bullard claims that women themselves don’t need to worry about prosecution, his explanation suggests otherwise: “It would not be after the woman unless the woman is herself the one trafficking that pill.” So…women won’t be targeted unless they break the law? How is that different than prosecuting anyone else?
Expect to see more legislation like this spread across anti-abortion states. Keep an eye out for language around “trafficking,” “controlled substances,” and especially “intent.”
In the States: Montana, South Carolina, Massachusetts, Texas & More
Let’s start with some good news out of Montana, where anti-abortion activists have lost their case challenging abortion protections in the state constitution. Again.
You see, this is the third attempt by the Montana Life Defense Fund to overturn the results of a 2024 ballot measure that codified abortion protections. Their claim is that voters were somehow misled into supporting Constitutional Initiative 128 because the full text of the amendment wasn’t printed directly on the ballot.
Last week, Yellowstone County District Judge Thomas Pardy rejected that claim, ruling that while the full text must be submitted to the Secretary of State, it does not need to appear on the ballot itself.
And let’s be real: this measure passed with overwhelming support. It was abundantly clear that Montana voters wanted abortion rights protected. But the argument that voters didn’t truly understand what they were voting for has become increasingly common since the end of Roe—especially as abortion rights ballot measures continue to win.
How many different ways can they say they don’t care what voters want?
In South Carolina, the local NAACP has come out against legislation that would classify abortion pills as a controlled substance. (H. 4760 passed the House in February.) The group warned:
“Regardless of where individuals stand on abortion, every South Carolinian should be troubled by any attempt to fast-track legislation involving critical healthcare medications without allowing medical professionals, impacted families, legal experts, clergy, and the public the opportunity to fully examine its consequences.”
Several states have moved to make abortion medication a controlled substance since Louisiana started the trend last year. And remember: putting abortion pills legally on par with addictive drugs like opioids doesn’t just increase criminal penalties—it also gives the state new ways to track who prescribes and uses the medication.
Over in Massachusetts, Gov. Maura Healey (who I was fortunate enough to sit on a panel with her a few weeks ago) is coming out strongly in defense of abortion pill access. During a Friday press conference, Healey urged the Supreme Court to “protect mifepristone” and “protect women’s access to healthcare in this country.”
"To be clear, this whole discussion, this whole debate, all these court cases, it’s all about an attack on women. That’s what it boils down to. Are you taking away women’s access to healthcare or not?"
Finally, the Houston Press reminds us that Planned Parenthood is still seeing patients in Texas, despite the state’s total abortion ban. While the organization has had to massively cut operations—Planned Parenthood Gulf Coast shuttered after nearly 100 years of operating in Texas—Planned Parenthood Greater Texas remains, and continues to serve more than 100,000 people every year.
Associate medical director Dr. Anitra Beasley said it’s no accident that many people believe Planned Parenthood has disappeared entirely from the state:
“All of the attacks against Planned Parenthood are very purposeful, so if the message can get out that we are closed, that’s the message some people want. We are still here and we still care. One of our slogans is ‘Planned Parenthood cares, no matter what.’ We’re here to give evidence-based, unbiased, patient-centered care.”
Quick hits:
AED in the News
I had a chance to chat about the attack on mifepristone with two of the smartest women around: Mini Timmaraju, president of Reproductive Freedom for All, and journalist Katie Phang, who hosted us on her (very cool!) show. Watch our conversation below:
Mifepristone Attacks 101
Need to catch up on the last week of attacks on mifepristone? We’ve got you covered. Since the Fifth Circuit ruling dropped, Abortion, Every Day has been tracking every legal development, political strategy, and anti-abortion talking point around abortion pills.
Start with our explainer on the ruling itself—and why it represents the most significant attack on abortion access in the last four years:
Then catch up on everything AED covered this past week as the fallout unfolded:
I also joined Katie Couric to talk through what all of this means—and shared the language, organizations, and resources people should be circulating to make sure everyone knows they can still get abortion pills by mail.
xxxxxxxxxxxxxxxxx
Missouri ‘born-alive’ abortion bill heads to governor after contentious House debate • Missouri Independent
Healthcare providers could face the death penalty if they don’t provide life-saving care to a baby born after an attempted abortion under legislation headed to Missouri Gov. Mike Kehoe.
The legislation — approved by the House Wednesday on a 102-46 vote — has been a top priority of Republicans this year and was the only significant anti-abortion bill to pass this year with just two days left in the legislative session.
The bill faced a Democratic filibuster earlier this year in the Senate. Last week it was given a second opportunity when the bill’s sponsor, Republican state Sen. Brad Hudson of Cape Fair, agreed to remove language seeking to open the door for lawsuits against anyone involved in an illegal abortion, including medication abortion, as part of a deal with Democrats to pass it through their chamber.
On Wednesday, Republican state Rep. Brian Seitz of Branson told his colleagues that the latest iteration of the bill, which he was handling, shouldn’t be controversial now that the civil liabilities language was removed.
“The Democrats are putting themselves in a very dangerous political position by not supporting healthcare for a living child,” Seitz told The Independent ahead of the vote.
Despite being presented a pared-down version of the bill, the House on Wednesday quickly became embroiled in heated debate over the legislation’s purpose and practicality.
House Minority Leader Ashley Aune, a Kansas City Democrat, called Seitz “a sad little man cosplaying as Superman when he’s not busy controlling women’s bodies.”
Seitz, who regularly wears ties with the Superman logo, responded by accusing Aune of “satanic mockery.” The exchange marked the culmination of a debate in which House Republicans accused their Democratic colleagues of condoning the killing of babies and Democrats accused Republicans of political theater.
Under the “Born-Alive Abortion Survivors Protection Act,” anyone who “knowingly performs or attempts to perform an overt act that kills a child born alive” can be charged with first-degree murder.
In 2024, voters enshrined the right to abortion up to the point of fetal viability in the Missouri Constitution. Viability is the point in pregnancy when a fetus can survive on its own outside the womb without extraordinary medical interventions.
Abortions are not currently being performed after the point of fetal viability in Missouri. With modern medical technology, it is exceedingly rare that an elective abortion performed after fetal viability ends in a birth.
Infanticide is illegal. But Republicans say the protections of the federal Born-Alive Infants Protection Act of 2002 doesn’t go far enough in dictating what kind of care a baby should be given.
Several Missouri OB-GYNs have testified against the legislation this year, saying it could force a hospital’s legal team to get involved before a doctor can treat complicated pregnancy diagnoses, including the diagnosis of fatal fetal anomalies in which families choose to induce an early labor.
“What the bill really is doing is creating a threatening environment for medical providers who both must follow the law as well as the standards of their practice,” state Rep. Pattie Mansur, a Kansas City Democrat, said Wednesday.
Democrats argue the bill could have a chilling effect on medical professionals in a state that recently saw a 25% drop in applicants for OB-GYN medical residencies.
State Rep. Connie Steinmetz, a Democrat from Maryland Heights, said the bill was an unwelcome invitation by lawmakers into doctors’ offices.
State Rep. Deanna Self, a Republican from St. Paul, disagreed.
“The government should be in the doctors’ office to do everything they can to protect life,” she said.
State Rep. Ken Jamison, a Democrat from Gladstone, called the bill a “disservice to unborn children,” claiming that Missouri lawmakers’ “misguided obsession with abortion has caused neglect of prenatal care.”
“Meanwhile, unborn children in Missouri are screaming from the womb for prenatal care,” said Jamison, emphasizing the state’s growing maternal healthcare deserts. “ … The greatest danger to unborn children is not abortion, it’s miscarriage.”
State Rep. Bryant Wolfin, a Republican from Ste. Genevieve, raised concerns that the bill is unconstitutional because the Senate version tacked on two amendments broadening the scope of the state’s Pregnancy-Associated Mortality Review Board and creating criminal provisions around cyberstalking.
Because of these additions, four Republicans voted against the bill last week, worried it violated a constitutional requirement that bills address a single subject “clearly expressed in its title.” Earlier this week, longtime anti-abortion lobbyist Sam Lee also declined to support the final bill, calling the changes a “poison pill” to the underlying legislation.
“Is the ‘Born-Alive Abortion Survivors Act’ worth taking that risk?” asked Wolfin, who was ultimately one of two Republicans to vote against the bill.

Melana Salisbury is among a small protest that breaks out in the Missouri House gallery as the House passed a “Born-Alive Abortion Survivors Protection Act,” bill Wednesday (Anna Spoerre/Missouri Independent). Just ahead of the vote, several protesters with Abortion Action Missouri rose from their seats in the House’s upper gallery, chanting “When abortion rights are under attack, what do we do? Stand up fight back.”
They were quickly escorted from the chamber.
Missourians will again vote on abortion later this year after lawmakers last session voted to put a new abortion ban on the ballot.
No comments:
Post a Comment