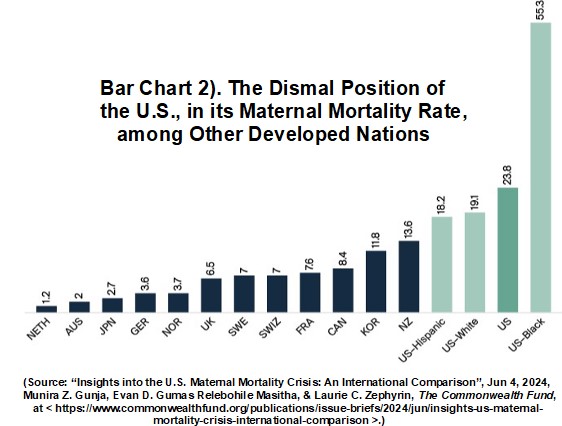
1). “Insights into the U.S. Maternal Mortality Crisis: An International Comparison”, Jun 4, 2024, Munira Z. Gunja, Evan D. Gumas, Relebohile Masitha & Laurie C. Zephyrin, The Commonwealth Fund, < https://www.commonwealthfund.
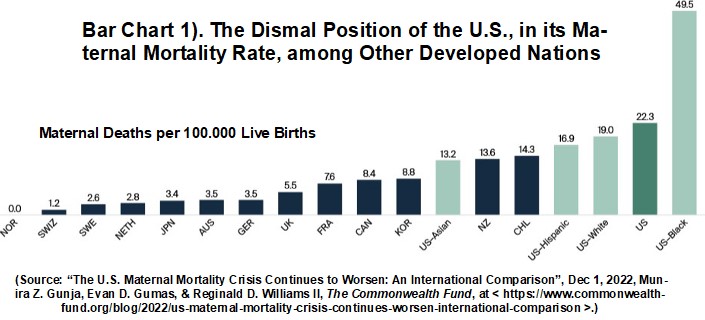
2). “The U.S. Maternal Mortality Crisis Continues to Worsen: An International Comparison”, Dec 1, 2022, Munira Z. Gunja, Evan D. Gumas, & Reginald D. Williams II, The Commonwealth Fund, < https://www.commonwealthfund.
3). “The Fury Gap: Young women were radicalized overnight”, Nov 07, 2024, Jessica Valenti, Abortion, Every Day, at < https://jessica.substack.com/
~~ recommended by dmorista ~~
Introduction by dmorista: The statement that 1,000 Women were tortured and murdered by the Forced-Pregnancy / Forced-Birth operatives sounds like a piece of Trumpian disinformation and hyperbole. And, if they were Trumpian blather, the right would be organizing forces to attack the perpetrators regardless of the imaginary reality of their propaganda memes. However, in this instance, the allegations are true. The Maternal Mortality rates in the U.S., were already dismal, even before the Discredited Partisan Hack U.S. Supreme Court handed down the Dobbs Decision. Item 1)., “Insights into the U.S. ….”, and Item 2)., “The U.S. Maternal Mortality Crisis ….”, both address these issues. Since the Dobbs Decision some 20 states now totally prohibit abortions and even enlightened states like California have a problem with Catholic Hospitals unilaterally making abortion unobtainable. In one notorious incident a woman who needed a prompt abortion was sent home from a Catholic Hospital in California with a bucket and some rags. She survived but was grievously harmed. A general observation was that 2/3 of U.S. Maternal Mortality takes place after birth, and the problem is made worse by nearly complete dearth of support for new mothers. All the other Advanced countries provide home visits and help to new mothers and fathers.
1,000 Women tortured & murdered
But the situations caused by Dobbs Decision, and the resultant Trump Abortion Bans, created new and unprecedented situations; with women undergoing extended torturous and horribly painful ordeals that sometimes lasted for several days. Some selected examples of these deadly ordeals were exposed by reports in ProPublica (now slated for retribution by the incoming Trump Fascist Regime). A few of these stories have been exposed by diligent journalism and brave families whose beloved female family members had been killed by the Forced-Pregnancy / Forced-Birth laws. There are totally reliable statictics the point out the the Maternal Mortality Rate in Texas climbed by 56%, and applying the previous Maternal Mortality Rate vs the new higher Maternal Mortality Rate and the Total number of live births in Texas in 2022, I found that an extra 42 women died. This lends itself to a rough extrapolation when the 12.5% increase in Maternal Mortality over the entire U.S. is examined the same way as I examined the Texas Maternal Mortality Rate changes in 2022. This large increase in women's deaths, is clearly the result of the Texas Bounty Hunter / Vigilante Abortion law, known as SB-08. It is not easy picking out the increases in the Maternal Mortality Rate that are due to changes in how statistics are kept or to general oppressive nature of the U.S. South. Texas has been busy appointing Forced-Pregnancy / Forced-Birth fanatics, like notorious anti-abortion crackpot OB/GYN Ingrid Skop to the state commission that controls the abortion statistics.
In Item 3)., “The Fury Gap: ….”, Jessica Valenti looks at the newly hardened attitudes of young women to men and sexual relationships as a result of the election. A new movement to eschew romantic interactions with men has arisen using S. Korean ideas the 4-B movement. CNN reports that:
“In the hours and days since it became clear that Donald Trump would be re-elected president of the United States, there’s been a surge of interest in the US for 4B.
“Young liberal women across TikTok and Instagram are discussing and sharing information about the South Korean feminist movement, in which straight women refuse to marry, have children, date or have sex with men.
“These women say they are enraged and fed up after a majority of their male counterparts voted for a candidate who was found liable for sexual abuse and whose appointment of three conservative Supreme Court justices led to the overturning of national abortion rights protections.
“In response, they say they’re swearing off men — and they’re encouraging others around the country to join them.
“ 'We have pandered and begged for men’s safety and done all the things that we were supposed to, and they still hate us,' Ashli Pollard, a 36-year-old in St. Louis, told CNN. ….
“4B is a shorthand for the four Korean words bihon, bichulsan, biyeonae and bisekseu, which translate to no marriage, no childbirth, no dating and no sex with men.
“The 4B movement emerged in South Korea around 2015 or 2016 ….
“In 2016, a woman was brutally killed near a Seoul subway station — the perpetrator reportedly said he killed her because he felt ignored by women.”
(See, “After Trump’s win, some women are considering the 4B movement”, Nov 9, 2024, Harmeet Kaur, CNN, at < https://www.cnn.com/2024/11/
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Insights into the U.S. Maternal Mortality Crisis: An International Comparison

Anna Ruocco (left), a midwife, provides home breastfeeding assistance to a mother with her newborn, on June 17, 2022, in Turin, Italy. Midwifery-led care models have been shown to provide care that is comparable to, or sometimes even better than, that provided by obstetrician-gynecologists, or ob-gyns. In the U.S., Canada, and Korea, ob-gyns outnumber midwives, while in most other countries midwives greatly outnumber ob-gyns. Photo by Diana Bagnoli/Getty Images
The U.S. maternal mortality rate continues to far exceed those of other high-income nations, despite a decline since the end of the COVID-19 pandemic
Persistent inequities in health care are a big reason why Black women in the U.S. are by far the most likely to die from pregnancy or childbirth
Introduction
The United States continues to have the highest rate of maternal deaths of any high-income nation, despite a decline since the COVID-19 pandemic. And within the U.S., the rate is by far the highest for Black women. Most of these deaths — over 80 percent — are likely preventable.1
With policies and systems in place to support women during the perinatal period, several high-income countries report virtually no maternal deaths. As policymakers and health care delivery system leaders in the U.S. seek ways to end the nation’s maternal mortality crisis, these countries may offer viable solutions.
This brief updates an earlier Commonwealth Fund study of differences in maternal mortality, maternal care workforce composition, and access to postpartum care and social protections between the U.S. and other high-income countries: Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, and the United Kingdom.2 In this edition, we have also included data on Chile, Japan, and Korea — all high-income countries with universal health care systems.
For our analysis, we used the most recently available data from the U.S. Centers for Disease Control and Prevention (CDC) and from the Organisation for Economic Co-operation and Development (OECD), of which the U.S. is a member. Where country-specific data are more than five years old, we note whether more recent published data from other sources are available for that country. Readers should be aware that because the methods we used to derive updated numbers from other sources may be different from methods the OECD uses, data points may not be comparable to the U.S. rates. For complete details on our methods, see “How We Conducted This Study.”
Highlights
- In 2022 there were approximately 22 maternal deaths for every 100,000 live births in the United States — far above rates for other high-income countries. U.S. maternal mortality is lowest for Asian American women and highest for Black women.
- Maternal death rates increased in Australia, Japan, the Netherlands, and the U.S. during the height of the pandemic, between 2020 and 2021. In Chile, Norway, and the U.S., where 2022 data are available, maternal death rates have begun to decline.
- Nearly two of three maternal deaths in the U.S. occur during the postpartum period, up to 42 days following birth. Compared to women in the other countries we studied, U.S. women are the least likely to have supports such as home visits and guaranteed paid leave during this critical time.
- The U.S. and Canada have the lowest supply of midwives and ob-gyns. In the U.S., Canada, and Korea, ob-gyns outnumber midwives.
Findings
Recent Maternal Mortality Trends
In 2022, there were 22 maternal deaths for every 100,000 live births in the U.S. — more than double, sometimes triple, the rate for most other high-income countries in this analysis. In half of the countries, there were less than five maternal deaths per 100,000 live births.
For Black women, maternal mortality is exceptionally high. Prior research has found Black people receive worse-quality care than white people on 52 percent of measures, including measures of care process, such as the ability to receive needed care; care outcomes, such as death; and patients’ perceptions of care.3
Other data show that racial disparities exist both within hospitals and between hospitals for maternal morbidity.4 Inequities in access to care and patients’ experience of care are often rooted in discrimination and clinician bias.5
The COVID-19 pandemic challenged health systems across the world and may have played a role in limiting women’s access to health care.6 The increase in maternal deaths in several countries during the pandemic may have been due to a rise in respiratory or viral conditions directly related to COVID or to conditions worsened by the virus, such as diabetes or cardiovascular disease.7 In addition, around the world, disruptions in health care delivery resulted in delayed or decreased access to needed maternal health care.8
During the height of the pandemic in 2020–21, maternal death rates increased in four of the nine countries shown in the chart above — Australia, Japan, the Netherlands, and the United States. These increases were higher in the U.S. for Hispanic women. It’s been well documented that the COVID-19 pandemic had a greater impact on Latino people, with one study finding that roughly a third of Latina maternal deaths were linked to COVID.9 In addition, lower vaccine uptake, especially among Black and Hispanic women, was found to be leading to more maternal deaths by the end of 2021.10 Owing to sample-size limitations, trends in annual mortality data for American Indian and Alaska Native women cannot be shown.
In Chile, Norway, and the U.S., for which 2022 data are now available, the maternal death rate has begun to decrease once again. In 2022, Norway’s maternal mortality rate was 0.11
The majority of deaths in the U.S. occur in the postpartum period, from one day after giving birth to a full year later. In the first week postpartum, severe bleeding, high blood pressure, and infection are the most common contributors to maternal deaths, while cardiomyopathy is the leading cause of late deaths.12
Still, more than one of five deaths occur during pregnancy itself, with heart conditions and stroke the leading causes.
Differences in Care During Pregnancy, Labor, and Delivery
Midwives are clinicians trained to provide a wide range of services — helping to manage normal pregnancies, assisting with childbirth, and providing care during the postpartum period, among others. In many countries, they are key providers of reproductive health care for women. A recent study found that a midwife workforce, integrated into health care delivery, could provide 80 percent of essential maternal care around the world and potentially avert 41 percent of maternal deaths, 39 percent of neonatal deaths, and 26 percent of stillbirths.13 By placing a priority on natural reproduction processes and relationship-building, midwives also can help address the social needs of mother, baby, and family.14
Midwifery-led care models have been shown to provide care that is comparable to, or sometimes even better than, that provided by obstetrician-gynecologists, or ob-gyns.15 In the U.S., Canada, and Korea, ob-gyns outnumber midwives, while in most other countries midwives greatly outnumber ob-gyns.
The U.S. and Canada have the lowest overall supply of midwives and ob-gyns — 16 and 13 providers per thousand live births, respectively. Nearly 7 million women in the U.S. currently live in counties where there are no hospitals or birth centers offering obstetric care and no obstetric providers, and the shortage is expected to only get worse in coming years.16
High-quality postpartum care is intended to ensure the physical and emotional recovery of mothers and their babies and can help reduce maternal deaths.17 Visits by a midwife or a nurse are associated with improved mental health and breastfeeding outcomes as well as reduced health care costs. Home visits give providers an opportunity to address maternal and mental health concerns as well as to assess the mother’s available supports and social drivers of health, including needs for food, housing, financial security, and protection from domestic violence.
All countries, apart from the U.S., guarantee at least one such home visit within one week postpartum, although Medicaid programs in some U.S. states cover these visits.
Paid maternity leave allows women to better manage the physiological and psychological demands of motherhood, helps ensure financial security for families, and leads to lower infant mortality.18 All countries included in this study, apart from the U.S., mandate at least 14 weeks of paid leave from work. Several countries provide more than a year of parental or home care leave. While U.S. states and employers can opt to provide paid leave, just over a quarter of American workers have access to paid family leave through either their employer or the state where they reside.19 In the U.S., women who are white and have higher incomes are more likely to take paid leave than Black women. Women who are able to take paid leave have lower rates of postpartum depression.20
Policy Implications
Black women continue to die from pregnancy and childbirth complications at unacceptably high rates, and U.S. women overall are more likely to die from maternal complications than women in other high-income countries. While the number of maternal deaths is lower in 2022 than in earlier years — primarily because there were fewer COVID-related maternal deaths — the United States faces continuing challenges in reducing maternal mortality.
Our findings suggest that an undersupply of maternity providers, especially midwives, and lack of access to comprehensive postpartum support, including maternity care coverage and mandated paid maternity leave, are contributing factors. Because both these factors disproportionately affect women of color, centering equity in any future policy changes will be a key to addressing the crisis.
Although overall maternal mortality rates in the other high-income countries we studied are lower than in the U.S., it should be noted that health inequities among women exist in these other countries, too.21 In the United Kingdom, for example, Black women are four times more likely to die than white women are.22 In Australia, Aboriginal women are about twice as likely as non-Aboriginal women to die from maternal complications.23
Midwifery Care
Outside the U.S., midwives are often considered the backbone of the reproductive health system. But the U.S. health system does not systematically incorporate midwives into the provision of essential maternity care services, even though these clinicians could improve the quality of care and experience of care for women, particularly women of color.
Some U.S. states have strengthened access to midwives and achieved positive outcomes, but midwifery services are not uniformly covered by private insurance plans across the country. While the Affordable Care Act (ACA) requires state Medicaid programs to cover midwifery care, Medicaid’s low provider reimbursement rates, coupled with a low supply of midwives, often mean that beneficiaries are unable to access these services.
Midwives also could help address maternity workforce shortages in the U.S., where nearly half of counties lack a single ob-gyn. An estimated 8,000 more ob-gyns are needed to meet demand — a number that may rise to 22,000 by 2050.24
Insurance Coverage
Universal, comprehensive maternity care coverage, along with exemptions from cost sharing, also are the norm in other high-income countries.25 The U.S. is the only one of these countries that does not have universal health care, leaving nearly 8 million women of reproductive age uninsured. The racial or ethnic groups that are the least likely to have health insurance and the most likely to face cost-related barriers to getting care are Black, Hispanic, American Indian and Alaska Native, and Native Hawaiian and other Pacific Islanders.26
The ACA’s expansion of eligibility for Medicaid coverage has been associated with better maternal health outcomes in the states that have opted in, particularly rates of maternal mortality for Black and Latina mothers.27 Ten states have yet to expand their Medicaid programs, leaving hundreds of thousands of women of reproductive age, disproportionately Black or Latina, in the Medicaid coverage gap and vulnerable to having their coverage terminated 60 days postpartum, as current policy allows. (Forty states have extended their postpartum Medicaid coverage, with several more states planning to do so.28) In addition to gaining postpartum support, expanding Medicaid would improve access to preconception health care for women of reproductive age who are in the Medicaid coverage gap.
The unwinding of the pandemic-era policy of continuous Medicaid enrollment — states restarted eligibility redeterminations in April 2023 — poses an imminent threat to pregnant and postpartum women, who stand to lose their health coverage during this critical period.
Postpartum Support
Since roughly two of three maternal deaths occur after birth, strengthening postpartum health services should be a priority. The World Health Organization recommends at least four health contacts in the first six weeks following birth, yet two of five U.S. women — more often than not younger, low-income, and uninsured — skip their one postpartum check-up.29 Eliminating barriers that cause people to skip postpartum visits is critical. In Chile, for example, conditional cash-transfer programs provide financial incentives to ensure that mothers can take advantage of health and social benefits, including home visits from midwives and nurses during the postpartum period. Such cash transfers have proven successful in increasing accessing to health services and reducing inequities within the country.30
The U.S. is the only high-income country that does not guarantee all mothers paid parental leave, although 13 states and the District of Columbia have introduced some mandatory paid leave, ranging from six to 12 weeks.31 A federally mandated paid leave policy would be especially beneficial to Black and lower-income women, who are less likely to have a paid leave policy through their employers.32
The well-being of mothers and babies should be a top policy priority in all countries. In the United States, which spends more on health care than any other high-income country, but has much worse maternal health outcomes, policymakers and delivery system leaders could learn a lot from international models of maternity care, including those related to postpartum support and workforce composition. In combination with equity-centered efforts, these examples could inspire the kind of reforms necessary to end the U.S. maternal health crisis.
OECD Data Analysis
This analysis used data from the 2023 release of health statistics compiled by the Organisation for Economic Co-operation and Development (OECD), which tracks and reports on a wide range of health system measures across 38 high-income countries. Data on paid maternity leave are from the OECD’s Family Database.33
Data on maternal mortality ratios, supply of midwives, and supply of ob-gyns were extracted in February 2024. While the information collected by the OECD reflect the gold standard in international comparisons, it may mask differences in how countries collect their health data. Full details on how indicators were defined, as well as country-level differences in definitions, are available from the OECD.
CDC Data Analysis
For U.S. maternal mortality data, we used the latest data from the U.S. Centers for Disease Control and Prevention (CDC) National Vital Statistics Systems, 2022. For timing of maternal deaths in the United States, we used the latest data from the CDC’s Maternal Mortality Review Committees in 36 states.34
While international data on timing of maternal and pregnancy-related deaths may be available, findings for the U.S. did not correspond with the latest CDC data. Because of potential data comparability concerns, we therefore omitted these findings from this data brief.
Data on postpartum home visits were compiled from a variety of country-specific sources, as specified in the notes on the exhibit.
Individual Country Data Updates
France: The latest OECD data for maternal mortality are from 2015. Other sources have confirmed the maternal mortality rate has stayed roughly the same, at eight maternal deaths per 100,000 live births.35
United Kingdom: The latest OECD data for maternal mortality are from 2017. Research from other studies has found the maternal mortality rate to have increased to 13.41 deaths per 100,000 live births over a three-year period (2020–2022).36 The methods used to derive this number may be different from that used for other countries and therefore may not be comparable in this analysis.
United States: OECD data regarding the supply of ob-gyns and midwives are from 2016. A 2022 report confirmed there are roughly 12 ob-gyns and four midwives per 1,000 live births in the U.S.37
The authors thank Chris Hollander, Aishu Balaji, Rachel Nuzum, Melinda Abrams, Arnav Shah, Faith Leonard, Jen Wilson, and Paul Frame, all of the Commonwealth Fund, for their help with this brief.
- There is insufficient evidence to understand which policy levers might have led to the decrease in maternal deaths in Norway. Interviews with experts revealed that no maternal health or other health policy changes were implemented after 2020. ↩
Maternal Mortality Rate in U.S. Worsens

Data show that the maternal mortality rate in the United States — more than three times the rate in most other high-income countries — is getting worse, and the rate for Black women is nearly three times higher than for white women
Deaths from complications related to pregnancy in the U.S. can be reduced by ensuring all women have access to primary care, expanding and diversifying the maternal care workforce, and providing access to comprehensive postpartum support
The maternal mortality rate in the United States has for many years exceeded that of other high-income countries. Data from the Organisation for Economic Co-operation and Development and the Centers for Disease Control and Prevention show rates worsening around the world in recent years, as well as a widening gap between the U.S. and its peer nations.
New international data show the maternal mortality rate in the U.S. continues to exceed the rate in other high-income countries. In 2020, the maternal mortality rate in the U.S. was 24 deaths per 100,000 live births — more than three times the rate in most other high-income countries. In the Netherlands, almost no women died from maternal complications.
The U.S. maternal mortality rate is exceptionally high for Black women. It is more than double the average rate and nearly three times higher than the rate for white women.
The U.S. maternal mortality rate has been on the rise since 2000 and has spiked in recent years. The COVID-19 pandemic challenged health systems across the world and may have played a role in limiting women’s access to health care. Consistent with this finding, when looking at countries where maternal mortality data are available since 2018, we find the U.S. is not alone. The maternal death rate increased in six of the nine countries shown. It is yet to be seen whether this trend in maternal deaths continued throughout the pandemic.
The maternal mortality rate dropped in Australia, Japan, and the Netherlands, although there is currently insufficient research to understand which policy levers may have caused these decreases. Research has shown that in the Netherlands there was an increase in home births and vaginal deliveries and a decrease in cesarean sections (both planned and emergency) during the pandemic. These practices may have contributed to lowering maternal deaths.
Focusing on Coverage and Postpartum Support
There are clear opportunities to put the U.S. on par with other countries that have implemented policies to help reduce maternal deaths. These strategies include: ensuring all women have access to free or affordable primary care; comprehensive reproductive health care before, during, and after pregnancy; a maternal health care workforce mainly comprising midwives covered by insurance; and comprehensive postpartum support.
The U.S. is the only country in this analysis that does not provide universal health care, leaving nearly 8 million women of reproductive age uninsured. Eleven states have yet to expand their Medicaid programs, leaving hundreds of thousands of women of reproductive age — who are disproportionately Black — in the Medicaid coverage gap and vulnerable to the current provision that allows states to end coverage 60 days postpartum.
The Biden administration’s proposal to extend Medicaid coverage to one year postpartum would provide millions of lower-income women with needed health care during the postpartum period, a time when many women die because of lack of adequate care. Comprehensive reproductive health coverage and other proposals from the administration, including expanding and diversifying the maternal care workforce, could decrease the number of preventable deaths and also reduce racial and ethnic inequities in U.S. maternal deaths.
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
The Fury Gap

If you thought the gender divide was bad before, you haven’t seen anything yet. Donald Trump’s win this week, bolstered by online shitposters and billionaire misogynists, has shifted something fundamental in young women. And while we’ll see plenty of ink spilled in election post-mortems about the online radicalization of young white men—as there should be—it would be a mistake to miss the story of how this election is doing something similar to their female counterparts.
Over the last two days, I’ve watched as young women’s TikToks and social media posts went from inconsolable shock to pure, hot rage. I saw in real time as those in their teens and 20s—some of whom voted for the first time—realized the depths of their country’s disdain for them.
For those of us in middle age or older, there wasn’t anything revelatory about the election; we’ve lived that betrayal for years. But to understand for the first time that America would rather elect a rapist than a woman is soul-crushing. Even worse: Realizing just how many men voted for Trump not in spite of his sexual predation—but because of it.
As difficult as that epiphany is to bear, it did not take long for this younger generation of women to respond with a resounding fuck that and fuck you. Notably, their anger isn’t at the world at large, but pointedly focused:
And then there’s this: In the hours after Trump was elected, Google search term interest in the ‘4B movement’ spiked—that’s a South Korean feminist term for women who swear off sex, marriage and childbirth with men.
I don’t think that’s a passing fad or empty threat.
Even before Roe was overturned, American women were getting married later and less. Knowing that so many of their male cohort voted for the serial abuser who stripped them of their rights isn’t likely to reverse this trend.
And let’s be clear: It’s not women who will suffer as a result of any Lysistrata-type protest.
For as much as American culture paints young women as marriage-crazed and desperate to land a man, the truth is that it’s actually men who want a wife and family. While only 45% of young women want to be mothers, 57% of young men want the same. And while young men are in the midst of a loneliness epidemic—with more than 60% of them single—the majority of single women have taken themselves off the dating market entirely. In part, it’s because of how common it is to be harassed on dates.
And that’s the thing. Women aren’t opting out of relationships with men simply because they’ve gained political power, financial independence and the ability to create full lives on their own. It’s men’s bad behavior driving them away.
This is a generation of young women who grew up online, seeped in a world of social media misogyny and trolls who comment on their bodies and demand they “make me a sandwich.” And that’s on top of getting the same lessons that women my age did—told to watch what you wear, when you walk, and who you trust.
So I have to imagine that after a lifetime of being expected to eat shit, waking up on Wednesday morning knowing that the men in your lives voted away your humanity made the decision to leave them behind pretty easy.
Especially considering how many took the mask off immediately after the election was called: Since Tuesday, young men have flooded women’s mentions with “your body, my choice”—a phrase that some even started shouting at little girls at school just a day later.
It’s that Republican-enabled impunity that will keep young women furious. Why put up with even a minute of it?
When conservatives started to panic about marriage and birthrates, they had the opportunity to make it more appealing for women to get married and have children. They could have fought for paid parental leave, subsidized childcare and taught men to be better partners. But in Christian patriarchy, men are never wrong and they certainly never need to change. Better to let misogyny run amok than give women an iota of respect.
The truth is that men—young and old—are terrified: They’re afraid of being alone, afraid of losing power, and afraid that they have no idea who they are if they can’t subjugate women.
That’s why as despairing as I feel about the election, I have hope. Because few things are more powerful than a nation of furious, free young women.
No comments:
Post a Comment