1). “Gen Z, millennial women face historic headwinds when it comes to their health: Report, Among the factors cited were the pandemic and harmful social media content”, Nov 30, 2023, Anne Flaherty, ABC News, at < https://abcnews.go.com/Health/
2). “Millennial, Gen Z Young Women Face Increased Threats to Health and Safety Compared With Peers in Previous Generations, Despite Better Education, Pay”, “New Report Details Unfulfilled Promise of Generational Progress”, Nov 30, 2023, Anon, Press Release and a useful summary of the statistics, Population Research Bureau, at < https://www.prb.org/news/
3). “LOSING MORE GROUND: REVISITING YOUNG WOMEN’S WELL-BEING ACROSS GENERATIONS”, Nov 30, 2023, Sara Srygley, Beth Jarosz, Mark Mather, Jenin Abu-Hashem, & Diana Elliott, POPULATION BULLETIN • VOL. 77, NO. 1, Population Research Bureau, This report is a follow-up to the 2017 “ 'Losing Ground' report and Index of Young Women’s Well-Being”, published by the PRB in that year.
4). “Maternal Mortality and Maternity Care in the United States Compared to 10 Other Developed Countries”, Nov 18, 2020, Roosa Tikkanen, Munira Z. Gunja, Molly FitzGerald, Laurie C. Zephyrin, The Commonwealth Fund, at < https://www.commonwealthfund.
5). “NOWHERE TO GO: MATERNITY CARE DESERTS ACROSS THE U.S. 2022 REPORT”, Healthy Moms Strong Babies, n.d., anon, The March of Dimes, at <https://www.marchofdimes.org/
6). Human Rights Crisis: Abortion in the United States After Dobbs, Apr 18, 2023, Anon, Human Rights Watch, at < https://www.hrw.org/news/2023/
~~ recommended by dmorista ~~
Introduction by dmorista:
The 5 generations of American women, discussed and graphically represented in these narratives, are defined in this manner:
Silent Generation: born 1928 to 1945
Baby Boom:born 1946 to 1964
Generation X: born 1965 to 1980
Millennial: born 1981 to 1999
Gen Z: born 2000 and later
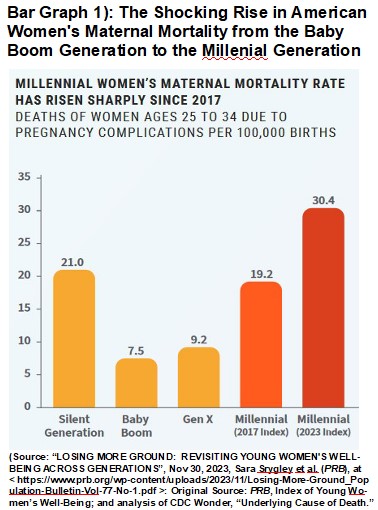
Some articles in the popular media, backed up by longer more technical reports have presented some shocking facts about American Health Care and the life prospects for Young American Women in general. Item 1). “Gen Z, millennial women ….”, reporting on the PRB study noted here in Item 2)., “Millennial, Gen Z Young Women ….”, and Item 3)., “LOSING MORE GROUND: ….”, points out that: “Maternal mortality among millennial women is some 30 deaths per 100,000, compared to 19 maternal deaths per 100,000 just a decade ago.” And Item 2). notes that: “.... Millennial women’s physical health and safety worsening over the past several years, threatened by rising suicide, homicide, and maternal mortality rates.” (Emphasis added)
However, as reported in Item 3, the increase in the Death Rate for pregnant women if we look a few years farther back is even more shocking. The Baby Boom generation of women had a Maternal Death rate per 100,000 women from 24 – 35 years of age due to pregnancy complications of only 7.5. For Millennial Generation women in 2023 this has risen to a stunning 30.4; or just slightly over 4 times as high. This is absolutely unprecedented in the history of the developed societies. See Bar Graph 1 below.
Another terrible trend is the increase in teen suicide rates among Young American Women and teenage girls. Item 1). reports that: “Among the most startling findings in the new report is the jump in suicide rates compared to past generations. When baby boomers were teens back in the 1960s and 1970s, for example, the suicide rate was 3 girls per 100,000. Now, Gen Z female teens experience an unprecedented rate of 5 per 100,000, according to the report.” Or in other words we have seen a tragic 67% increase in the suicide rate for teenage girls in the U.S.
These situations are unprecedented declines in the health of young people in the U.S., overwhelmingly caused by the relentless attacks by the reactionary minions of Finance Capital on the educational, social welfare, and other social service insitutions of American Society, pushing the U.S. into a “Third-World” level of human well-being.
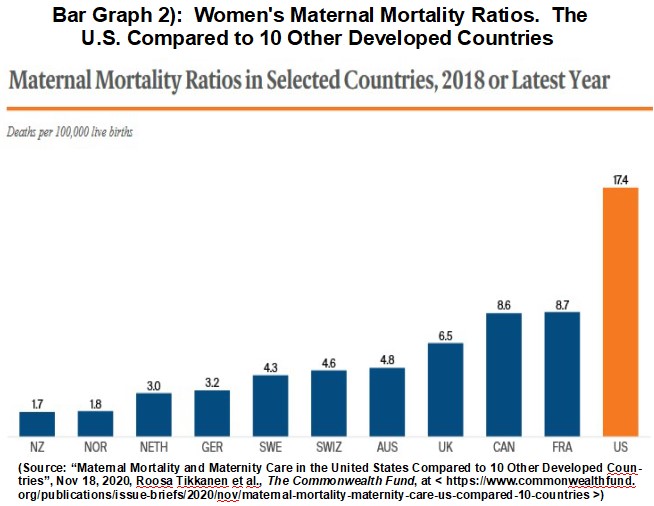
The dismal conditions for pregnant women in the U.S. are also discussed in Item 4)., “Maternal Mortality and Maternity Care ….”, that compares the U.S. to 10 other developed countries. The U.S. has a Maternal Mortality rate fully 10 times higher than that of New Zealand the country with the lowest rate among the 11 countries. Even France, the society with next worse Maternal Mortality rate to that of the U.S., had a rate only half that of the U.S. See Bar Graph 2 below. As far as I know Japan would likely have the lowest Maternal Mortality rate of any place on earth making the U.S. look even worse. The 10 countries chosen to compare to the U.S. were not selected for having the lowest death rate, but to represent a range of developed societies with a variety of statistics.
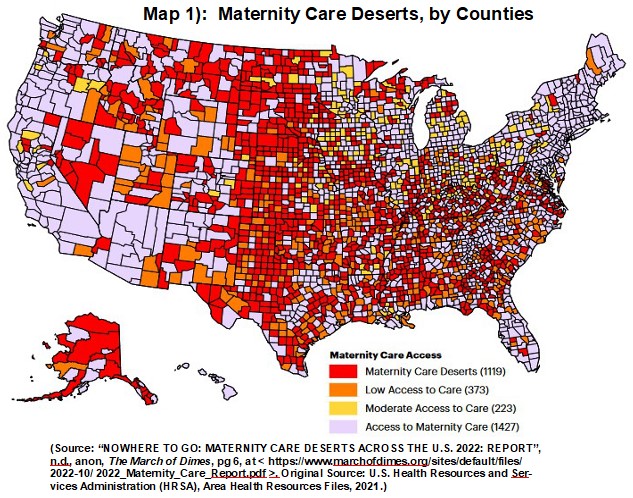
Some other aspects of the increasingly dire health care circumstances in which many American women live is discussed in Item 5)., “NOWHERE TO GO: MATERNITY CARE DESERTS ….”. The report discusses many aspects of the Reproductive Health Care situation found in the current day U.S. Looking at the red counties, displayed in a map in that article, and here shown as “Map 1): Maternity Care Deserts, by Counties”, we can clearly see that much of the reason that these 1,119 places are “deserts”, is that there is no major or medium sized city in those counties. MaternityCare is available in all the large and medium sized cities of the U.S., though clearly the quality of the care is clearly seriously compromised in the 20+ Red States that have passed draconian abortion bans. In those places women either return home, or languish in their cars in the parking lots, waiting to become sick enough to qualify for an abortion in those retrograde states. Perhaps we need a new classification and color code for counties where women can see facilities that provide some limited Maternal Care from the windows of their cars but cannot access it in a timely manner. All while over zealous police and prosecutors search their use of Menstrual Cycle apps, e-mails, cell-phone calls, and internet searches; looking for evidence the women are planning to flee to a Blue State for Reproductive Health Care.
(Please note that Freeze Peach previously posted the same map, as Map 1 here, “Map 1): Maternity Care Deserts, by Counties”, in the comment thread in response to my TCS article post “OB/GYNs and other College Grads: Red State Brain Drain ~~ Timothy Noah”, Nov 30, 2023, at < https://ongoingclassstruggle.
Another aspect of access to any sort of Health Care is being able to pay for the care. This report notes on page 21 that:
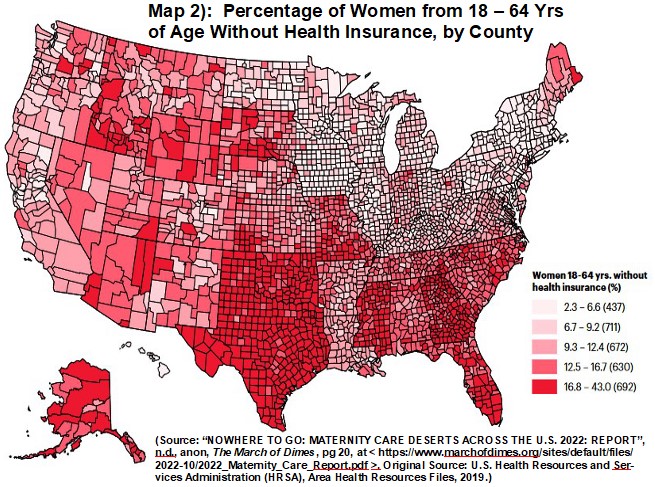
“The proportion of uninsured women ranges from 2.3 percent (Norfolk, Massachusetts) to 43 percent (Hidalgo, Texas). Massachusetts has the lowest proportion of uninsured women with a state average of 3.5 percent, while Texas has the highest proportion with an average of 23.3 percent uninsured women.”
The national situation is demonstrated well by a map from the March of Dimes report, posted here as Map 2 below. Texas, Oklahoma, Mississippi, Georgia, and Florida stand out as the states with the most severe problem in which a high proportion of women, from 18 – 64 years of age, who do not have health care insurance. This has ramifications beyond Reproductive Health Care.
Finally Human Rights Watch published a blistering criticism of the U.S. in Item 6)., “Human Rights Crisis: Abortion in the United States ….”. A report that opens with this Paragraph:
“I. Executive Summary ....
“Following the United States (US) Supreme Court decision in Dobbs v. Jackson Women’s Health Organization in June 2022, people in the US who can become pregnant (1) are facing an unprecedented human rights crisis. In Dobbs, the Supreme Court overturned the constitutionally protected right to access abortion, leaving the question of whether and how to regulate abortion to individual states. Approximately 22 million women and girls of reproductive age in the US now live in states where abortion access is heavily restricted, and often totally inaccessible. This briefing paper details the intensifying human rights emergency caused by the decision, and discusses the ways that Dobbs contravenes the US’ international human rights obligations.” (Emphasis added)
The report continues to enumerate the many horrific situations caused by the repeal of Roe v. Wade in very uncompromising language a couple more quotes are here below.
“II. Factual Background
“As of January 17, 2023, abortion is banned, with extremely limited exceptions, in thirteen states: Alabama, Arkansas, Idaho, Kentucky, Louisiana, Mississippi, Missouri, Oklahoma, South Dakota, Tennessee, Texas, West Virginia, Wisconsin, and Oklahoma. (4) Georgia has banned abortion after six weeks of pregnancy (effectively outlawing access entirely). (5) Approximately 22 million women and girls of reproductive age (ages 15-49) in the US live in states where abortion access is heavily restricted, and often totally inaccessible. (6) Four states have begun restricting access to medication abortions, including by prohibiting the mailing of medication into their jurisdictions. (7) Meanwhile, at least three states (Texas, Oklahoma, and Idaho) enacted so-called “bounty” laws before the Dobbs decision, empowering private citizens to sue providers who carry out abortions. (8) In continuation of the country’s devaluation of the lives of Black and Brown women, communities of color and of lower socio-economic status are bearing the brunt of these laws. (9) Dozens of clinics have closed across the country since Dobbs was decided, (10) increasing travel time and distance for women seeking care — and barring access for those women unable to travel. (11) ….
“4). These interviews and documentation by women’s rights groups describe difficulty, including:
in accessing abortion in cases of miscarriage;
forced travel across state lines in emergencies;
denial of care in cases of ectopic pregnancy;
hospitals delaying care until the woman’s health has deteriorated to a level most certainly to fit within narrow and vague “risk to life of the mother” exceptions;
professionals withholding information fearing that their advice could violate anti-abortion laws;
reduced access to non-reproductive healthcare (e.g. chemotherapy);
the infliction of serious psychological harm on women and girls forced to carry an unwanted pregnancy;
complications for adolescents forced to give birth;
reduced access to other forms of reproductive healthcare including contraception;
heightened risk of violence faced by pregnant individuals in abusive relationships; and
pregnant individuals forgoing prenatal care to avoid surveillance. ….
“15). Girls and adolescents are at increased risk of life-threatening consequences owing to delayed reproductive healthcare. Because girls and adolescents experience serious pregnancy-related complications at a higher rate than adults, (39) including, trauma to organs, (40) pregnant adolescents are particularly at risk when healthcare providers delay care. Despite this heightened vulnerability, none of the state abortion bans recognize an exception specifically for adolescent pregnancy. (41) Even before Dobbs, young people under 18 in at least 36 states faced “parental involvement” requirements forcing them to notify and/or seek permission from a parent to get an abortion. These restrictions remain in place in more than 20 states where abortion is still legal. (42)”.
The litany of outrages listed by Human Rights Watch is very long.
xxxxxxxxxxxxxxxxx
Gen Z, millennial women face historic headwinds when it comes to their health: Report
Among the factors cited were the pandemic and harmful social media content.

Progress in women's health since the 1960s is backsliding, with millennial and Gen Z women facing heightened risks to their physical well-being and safety compared to their moms or grandmothers, according to a report released on Thursday by the Population Reference Bureau.
The analysis, which looked at how women in their 20s and early 30s fared across generations, found that women born after 1981 are more likely to be at risk of suicide, death in childbirth and being murdered than young women in previous generations.
The findings come even as younger generations of women are also more likely to have access to better educational opportunities and higher pay than their parents, according to the report.
MORE: US life expectancy rose in 2022 due to fewer deaths linked to COVID-19: CDC
“Young women today are obtaining college degrees and entering the workforce in record numbers to achieve their generation’s version of the American Dream. But structural barriers to health and safety are preventing many of them from reaching their full potential,” said Diana Elliott, vice president for U.S. programs at the Population Reference Bureau.
As reasons for why millennial and Gen Z women are struggling more, the organization cited the rise of harmful social media content, the lingering impacts of the COVID-19 pandemic, increased political divisions and rising inflation. It also blamed restrictions on reproductive health access for young women, including state abortion restrictions.
The report defines millennials as born between 1981 and 1999; Gen Z are born 2000 and later.

“Increased rates of suicide and homicide, and a lack of access to health care services like safe abortion, have the combined effect of reversing the health and safety gains women of previous generations experienced, especially women of color," said Elliott.
The Population Reference Bureau, a nonprofit research organization that partners with the U.S. Census Bureau to examine issues of gender and poverty, is funded by several philanthropies like the Bill & Melinda Gates Foundation and MacArthur Foundation.
Among the most startling findings in the new report is the jump in suicide rates compared to past generations. When baby boomers were teens back in the 1960s and 1970s, for example, the suicide rate was 3 girls per 100,000. Now, Gen Z female teens experience an unprecedented rate of 5 per 100,000, according to the report.
Deaths in childbirth have also soared, the analysis found. Maternal mortality among millennial women is some 30 deaths per 100,000, compared to 19 maternal deaths per 100,000 just a decade ago.
On the upside, women are significantly more likely to get a collect degree, according to the report -- nearly 44% of millennial women compared to 28% of Generation X women. Incarceration rates are also declining for the first time in 50 years among women
xxxxxxxxxxxxxxxxxxxxx
Millennial, Gen Z Young Women Face Increased Threats to Health and Safety Compared With Peers in Previous Generations, Despite Better Education, Pay

Date
November 30, 2023
New Report Details Unfulfilled Promise of Generational Progress
WASHINGTON, D.C. – Progress for today’s young women—those primarily ages 25 to 34 in 2019-2021—has declined in comparison to those before them, according to a new report by Population Reference Bureau, “Losing More Ground: Revisiting Young Women’s Well-Being Across Generations.” The report details how young women’s lives in the United States have been upended in recent years, from the COVID-19 pandemic; to the Dobbs decision overturning Roe v. Wade’s reproductive health protections; to increased political divisiveness, rising inflation, and the impacts of social media. Where data are available, the report includes new insights on the teenage girls of Gen Z (born in 2000 or later). The analysis presents an updated picture of Millennial women’s health and well-being relative to women of the same age from Generation X, the Baby Boom, and the Silent Generation.
The data show that despite decades of progress between the 1960s and 1990s, each successive generation of women in the United States no longer does better than prior generations. This promise of progress began waning with Generation X and has continued to decline, with Millennial women’s physical health and safety worsening over the past several years, threatened by rising suicide, homicide, and maternal mortality rates.
“Young women today are obtaining college degrees and entering the workforce in record numbers to achieve their generation’s version of the American Dream. But structural barriers to health and safety are preventing many of them from reaching their full potential,” said Diana Elliott, Vice President for U.S. Programs, Population Reference Bureau. “Increased rates of suicide and homicide, and a lack of access to health care services like safe abortion, have the combined effect of reversing the health and safety gains women of previous generations experienced, especially women of color.”
Key Findings
- Among women ages 25 to 34, suicide rates have climbed from 4.4 deaths per 100,000 for Generation X to 7 deaths per 100,000 for Millennial women. While suicide rates have declined among young white women, they have increased for young women of color; American Indian and Alaska Native young women face a suicide rate 3 times that of their white peers.
- For Millennial women ages 25 to 34, maternal mortality rates have surged, from 19.2 deaths per 100,000 live births in 2013-2015 to 30.4 deaths per 100,000 live births in 2019-2021.
- The homicide rate for Millennial women ages 25 to 34 has increased to 4.5 deaths per 100,000 women compared to 4.3 deaths for Generation X women of the same age, reversing a trend of generational improvement previously seen in 2017. The homicide rate is particularly stark for Millennial Black women, at 14 deaths per 100,000 women in 2019-2021 compared to 9 per 100,000 in 1999-2001—a nearly 60% increase.
These health and safety declines are occurring despite young women’s progress on several indicators of economic well-being and their labor force participation remaining steady or improving across generations.
- The share of women with at least a bachelor’s degree has increased, with 43.6% of young Millennial women completing a college education compared to 28% percent of their Generation X peers, though gaps persist by race and ethnicity.
- The incarceration rate for women has declined for the first time in more than 50 years, falling 19% to 69.7 women in prison per 100,000 during the 2019-2021 period compared to 86 per 100,000 when Generation X women were young adults (1999-2001).
- Millennial young women’s earnings as a percentage of men’s have increased compared to the wages of their Generation X peers, rising from 82.4 cents per dollar to 89.7 cents per dollar.
About the PRB Index of Young Women’s Well-Being
Population Reference Bureau (PRB) first sounded the alarm on the decline in generational progress with its 2017 “Losing Ground” report and Index of Young Women’s Well-Being, describing how young women’s progress had stalled since the Baby Boom generation. The 2023 analysis “Losing More Ground” shows that Millennial young women’s well-being is declining as they experience more economic uncertainty and threats to their physical well-being than their peers in past generations. Despite improvements in women’s economic well-being, young women and men today both report high levels of stress related to inflation, money, housing costs, and the economy.
Defining the Generations
In “Losing More Ground,” PRB studies women primarily ages 25 to 34 in each generation. While generational definitions can differ slightly by source, PRB uses the following:
- Silent Generation: born 1928 to 1945
- Baby Boom:born 1946 to 1964
- Generation X: born 1965 to 1980
- Millennial: born 1981 to 1999
- Gen Z: born 2000 and later
About Population Reference Bureau
PRB is a nonpartisan, not-for-profit research organization focused on improving people’s health and well-being through evidence-based policies and practices. To learn more, visit www.prb.org. Follow us on X @PRBdata and on LinkedIn.
xxxxxxxxxxxxxxxxx
Maternal Mortality and Maternity Care in the United States Compared to 10 Other Developed Countries

The U.S. has the highest maternal mortality rate among developed countries
Many factors contribute to the high number of maternal deaths in the U.S., including too few maternity care providers, especially midwives, and lack of access to comprehensive postpartum supports
Abstract
- Issue: Most maternal deaths are preventable, but they have been increasing in the United States. Other high-income countries with success in preventing maternal deaths offer potential lessons for the U.S.
- Goals: To compare maternal mortality rates in the U.S. with 10 other high-income countries and identify differences in maternal care workforces, postpartum care access, and paid maternity leave policies that may help account for observed differences.
- Methods: Analysis of the latest data from the Centers for Disease Control and Prevention, Organisation for Economic Co-operation and Development, and grey literature.
- Key Findings: The U.S. has the highest maternal mortality rate among developed countries. Obstetrician-gynecologists (ob-gyns) are overrepresented in its maternity care workforce relative to midwives, and there is an overall shortage of maternity care providers (both ob-gyns and midwives) relative to births. In most other countries, midwives outnumber ob-gyns by severalfold, and primary care plays a central role in the health system. Although a large share of its maternal deaths occur postbirth, the U.S. is the only country not to guarantee access to provider home visits or paid parental leave in the postpartum period.
- Conclusion: The U.S. has a relative undersupply of maternity care providers, especially midwives, and lacks comprehensive postpartum supports.
Background
Although most are preventable, maternal deaths have been increasing in the United States since 2000.1 As U.S. policymakers and health care delivery system leaders seek ways to reverse this trend, countries that have achieved lower maternal mortality rates may offer possible solutions.
This issue brief provides an overview of differences in maternal mortality, maternal care workforce composition, and access to postpartum care and social protections in the U.S. compared to 10 other high-income countries: Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, and the United Kingdom.2 We use the most recently available data from the Centers for Disease Control and Prevention (CDC), the Organisation for Economic Co-operation and Development (OECD), and earlier Commonwealth Fund studies.3
Maternal Mortality and Timing of Deaths
Women in the U.S. are the most likely to die from complications related to pregnancy or childbirth.
In 2018, there were 17 maternal deaths for every 100,000 live births in the U.S. — a ratio more than double that of most other high-income countries (Exhibit 1). In contrast, the maternal mortality ratio was three per 100,000 or fewer in in the Netherlands, Norway, and New Zealand.
What We Mean by Maternal Mortality4
There are three commonly used measures of maternal deaths in the United States. While they all capture some aspect of maternal deaths, they are not equivalent.
Pregnancy-associated death: Death while pregnant or within one year of the end of the pregnancy, irrespective of cause.
Pregnancy-related death: Death during pregnancy or within one year of the end of pregnancy from a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition by the physiologic effects of pregnancy. Used in the U.S. only, this CDC measure is typically reported as a ratio per 100,000 births.
Maternal mortality: Death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes. Used by the World Health Organization (WHO) in international comparisons, this measure is reported as a ratio per 100,000 births.
A relatively large share of pregnancy-related deaths in the U.S. occur after birth.
To better understand the high maternal death rate in the U.S., it is helpful to know when they happen.
- Around one-third of U.S. pregnancy-related deaths, counted up to one year postbirth, occur during pregnancy (Exhibit 2).
- 17 percent of deaths occur on the day of delivery.
- 52 percent occur after delivery, or postpartum:
- 19 percent of all maternal deaths occur between one and six days postpartum.
- 21 percent of all maternal deaths are between one and six weeks postpartum.
- 12 percent of all maternal deaths take place during the remaining portion of the year; these are also known as late maternal deaths.5
In the first week postpartum, severe bleeding, high blood pressure, and infection are the most common contributors to maternal deaths, while cardiomyopathy is the leading cause of late deaths.6 Previous research indicates that U.S. women experience more late maternal deaths than women in other high-income countries.7
Differences in Care During Pregnancy, Labor, and Delivery
The U.S. has an overall shortage of maternity care providers relative to the number of births.
Midwives in many countries are key care providers trained to provide a wide range of services. Among these are helping to manage a normal pregnancy, assisting with childbirth, and providing care during the postpartum period. Placing a priority on natural reproduction processes and relationship-building, midwives also can help address the social and personal needs of mother, baby, and family.8 Ob-gyns, meanwhile, are physicians trained to identify and intervene in abnormal conditions that come up before, during, and after pregnancy. They typically provide care in hospital-based settings.
Midwifery-led care models have been shown to provide care that is comparable to, or sometimes even better than, that provided by obstetrician-gynecologists, or ob-gyns (see box).9
The U.S. and Canada have the lowest overall supply of midwives and ob-gyns — 12 and 15 providers per 1,000 live births, respectively (Exhibit 3). All other countries have a supply that is between two and six times greater.
What Does the Evidence Say About the Relationship Between Midwifery Care and Birth Outcomes?
The World Health Organization (WHO) recommends midwives as an evidence-based approach to reducing maternal mortality.10 Several systematic reviews have found that midwifery-led care for women with healthy pregnancies is comparable or preferable to physician-led care in terms of11:
- Maternal (mother) and neonatal (baby) outcomes, including lower maternal mortality and morbidity and reduced stillbirths and preterm births.
- More efficient use of health system resources, including lower use of unnecessary and potentially harmful interventions like C-sections for low-risk deliveries, epidurals, and instrument-assisted births.
- Improved patient satisfaction and maternal psychosocial well-being outcomes, including those for postpartum depression.
Some experts note that “high-income countries with the lowest intervention rates, best outcomes, and lowest costs have integrated midwifery-led care” into their health care systems.
Cross-Country Differences in the Type and Supply of Maternity Care Providers
In the U.S. and Canada, ob-gyns outnumber midwives. The American College of Nurse Midwives claims that the “U.S. maternity workforce is upside down relative to patient needs,”12 noting that the majority of births are low-risk and could be managed by midwives, family practitioners, or general practitioners.13 In several countries, including Canada, France, and New Zealand, primary care physicians also play a large role (although comparative international data are lacking).
In most other countries, however, midwives greatly outnumber ob-gyns. For example, midwives provide most prenatal care and deliveries in the U.K. and the Netherlands14 — countries considered to have among the strongest primary care systems in Europe.15 Dutch midwives also deliver home births, which represent 13 percent of all births, the highest rate of any developed countries.16
In some countries, women can choose their maternity care provider, as both midwife and obstetrician care services are covered by universal health insurance. In England, care may be shared between midwives and obstetricians.17
In the U.S., midwife services are not uniformly covered by private insurance plans. This is particularly the case when services are provided in nonhospital settings, like the home or a birthing center.18 And while the Affordable Care Act (ACA) requires that state Medicaid programs cover midwifery care, the supply of providers is often so low that beneficiaries are often unable to access these services. Several factors, which can vary widely from state to state, may be limiting the supply of midwives in the U.S. Among these are the state licensure laws, restrictive scope-of-practice laws, and rules requiring physician supervision of midwives.19
Maternal Care After Delivery
Access to home visits after delivery varies in the U.S. but is guaranteed in other countries.
Postpartum care is intended to ensure the physical and emotional recovery of mothers and their babies.20 Home visits by a midwife or a nurse are associated with improved mental health and breastfeeding outcomes as well as reduced health care costs.21 All countries, apart from the U.S., guarantee at least one such visit within one week postpartum, although some U.S. states provide these for Medicaid beneficiaries (Exhibit 4).22 Home visits give providers an opportunity to address mental health concerns and allow them to assess social determinants of health, including needs for food, housing, financial security, and protection from domestic violence.23
The U.S. is the only high-income country that does not guarantee paid leave to mothers after childbirth.
Maternity leave helps women manage the physiological and psychological demands of motherhood and helps ensure financial security for families.24 All countries included in this study, apart from the U.S., mandate at least 14 weeks of paid leave from work. And several countries provide more than a year of maternity leave (Exhibit 5).
Policy Implications
While the reasons behind the high U.S. maternal mortality rate are multifaceted, our findings suggest that an undersupply of maternity providers, especially midwives, and lack of access to comprehensive postpartum supports are contributing factors.
Midwifery care. In most countries, maternity care is well integrated with other primary care, and midwives play an important role. Some U.S. states have strengthened access to midwives and achieved positive outcomes.25 During the COVID-19 pandemic, as demand for midwifery care has grown in the U.S. (as it has around the world), several states issued emergency orders expanding midwifery services to pregnant women, including Maine, New Jersey, and New York.26
While the ACA requires Medicaid to pay for midwifery care provided in freestanding birth centers, more needs to be done to expand access to services and make them more affordable. Among the key issues to address are state variations in scope-of-practice rules for health care practitioners, low reimbursement rates for midwives, and payment parity.27
Countries also have rapidly reorganized their maternity care delivery systems during COVID-19 to expand use of telemedicine and the capacity to provide home births.28 To strengthen maternity care during the pandemic, the U.S. could look to countries with long-standing experience in home births and midwifery-led care.
Insurance coverage. Universal, comprehensive maternity care coverage, along with exemptions from cost-sharing, also are the norm in other high-income countries.29 While the ACA strengthened maternity care coverage, access to benefits often depends on type of insurance and geographic location, and out-of-pocket costs vary significantly as well.30
How the Affordable Care Act Has Helped Women Gain Access to Maternity Care
- Guaranteed issue: Insurers are no longer allowed to deny coverage to individuals who apply for insurance, including those with preexisting conditions.* Preexisting conditions specific to women include pregnancy, having had a C-section, and having been a victim of rape or domestic violence.
- Community rate-setting for premiums: Insurers are no longer allowed to charge women higher health care premiums than they charge men. This was a previously common practice, as women were anticipated to have higher health care costs, especially around child-bearing years. Because of the ACA, insurers are only allowed to charge higher premiums based on age and tobacco use.*
- Free preventive services: Insurers must provide preventive services such as breast cancer screening, cervical cancer screening, FDA-approved contraceptives, and osteoporosis and chlamydia screening for women in at-risk age groups, without copayments, coinsurance, or other cost-sharing.*
- Essential health benefits: All individual marketplace or small-group insurance plans must cover 10 essential health benefits,* including maternity coverage.
- Support for new mothers: Employers with at least 50 workers must allow nursing women reasonable breaks from work to express breast milk and must provide a private place to do so for the first year after a child’s birth.
- Expanded Medicaid eligibility: Individuals with incomes up to 138 percent of the federal poverty level can enroll in Medicaid, though this has been left up to states’ discretion.* Thirty-eight states and the District of Columbia have opted to expand their Medicaid program.
- Premium subsidies for low-income women: Premiums subsidies are available for all individuals earning up to 400 percent of the federal poverty level ($51,040 for an individual and $104,800 for a family of four in 2020) for the purchase of individual marketplace coverage.*
- Coverage for young women: Young adults can stay on a parent’s plan until their 26th birthday.* Before the ACA, young women 19 to 25 were uninsured at some of the highest rates.31
- Use of nurse midwives and freestanding birth centers: State Medicaid programs must include both as covered benefits. In addition, reimbursement for midwives was increased to the amount physicians receive for providing the same service.
- Creation of Maternal, Infant, and Early Childhood Home Visiting Program: Some 154,000 parents and children in 1,005 U.S. counties receive home visits through the program.32
* Also applies to men.
Postpartum care. Since more than half of maternal deaths occur after birth, strengthening postpartum care should be a priority. The World Health Organization recommends at least four health contacts in the first six weeks, yet U.S. women typically have a single office-based physician visit within this period, and some don’t have one at all.33
Expanding eligibility for Medicaid, which pays for 43 percent of U.S. deliveries, can lead to more stable postpartum coverage.34 Currently, however, the program’s coverage extends to only six weeks postpartum. Some states are expanding coverage up to one year, in line with recommendations by maternal mortality review committees and others.35
Paid leave. The U.S. is the only high-income country that does not guarantee all mothers paid maternity leave,36 although a few states have recently introduced some paid leave.37 Women receiving paid leave use fewer health care services compared to women with only unpaid leave.38
Racial disparities. The high maternal mortality rate in the U.S. masks dramatic variation by race and ethnicity: the number of deaths per 100,000 births for black non-Hispanic women in 2018 (37.1) was more than two times higher than that for white mothers (14.7). Hispanic women have the lowest rate (11.8).39 The pandemic has the potential to exacerbate existing U.S. racial disparities in maternal outcomes, as Black and Latino people have faced higher rates of economic hardship and mental health problems during the pandemic compared to their white counterparts.40
These disparities are not unique to the U.S., however. In the U.K., which has universal health coverage, maternal deaths were five times more common among Black women in the prepandemic period and two times more common among Asian women.41 Achieving equity in maternal outcomes remains a global challenge.
The well-being of mothers and babies should be a top policy priority in all countries. In the U.S., where maternal health outcomes are poor relative to many other parts of the world, policymakers and delivery system leaders can examine international models of maternity care to inform strategies for improvement.
How We Conducted This Study
This analysis used data from the 2020 release of health statistics compiled by the Organisation for Economic Co-operation and Development (OECD), which tracks and reports on a wide range of health system measures across 37 high-income countries. Data on maternal mortality ratios, supply of midwives, and supply of ob-gyns were extracted in August 2020. While the information collected by the OECD reflect the gold standard in international comparisons, it may mask differences in how countries collect their health data. Full details on how indicators were defined, as well as country-level differences in definitions, are available from the OECD.
We used the latest data from the Centers for Disease Control and Prevention’s (CDC) Pregnancy Mortality Surveillance System on the timing of maternal deaths in the U.S. While international data are available regarding timing of maternal and pregnancy-related deaths, findings for the U.S. did not correspond with the latest data from the CDC. Because of potential data comparability concerns, we omitted these findings from our formal analysis.
Data on postpartum home visits were compiled from a variety of country-specific sources, as specified in the notes to Exhibit 4, including a series of patient vignettes of a healthy 23-year-old woman who is pregnant for the first time, funded by the Commonwealth Fund and published in the New England Journal of Medicine in 2015.42
Data on paid maternity leave are from the OECD’s Family Database.
The 10 comparator countries included in this brief represent those high-income countries that take part in the Commonwealth Fund’s annual International Health Policy Survey: Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, and the United Kingdom.
Acknowledgments
The authors wish to thank Dr. Jodie D. Katon, Dr. Eugene Declercq, and Reggie Williams II for their helpful review comments; and Jesse Baumgartner and Gabriella N. Aboulafia for their careful data review.
1. Lauren M. Rossen et al., “The Impact of the Pregnancy Checkbox and Misclassification on Maternal Mortality Trends in the United States, 1999–2017,” Vital and Health Statistics, series 3, no. 44 (National Center for Health Statistics, Jan. 2020); Marian F. MacDorman et al., “Recent Increases in the U.S. Maternal Mortality Rate: Disentangling Trends from Measurement Issues,” Obstetrics and Gynecology 128, no. 3 (Sept. 2016): 447–55; Building U.S. Capacity to Review and Prevent Maternal Deaths: Report from Nine Maternal Mortality Review Committees (Maternal Mortality Review Information Application and Review to Action, 2018); and Emily E. Petersen et al., “Vital Signs: Pregnancy-Related Deaths, United States, 2011–2015, and Strategies for Prevention, 13 States, 2013–2017,” Morbidity and Mortality Weekly Report 68, no. 18 (May 10, 2019): 423–29.
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Human Rights Crisis: Abortion in the United States After Dobbs

I. Executive Summary
Following the United States (US) Supreme Court decision in Dobbs v. Jackson Women’s Health Organization in June 2022, people in the US who can become pregnant[1] are facing an unprecedented human rights crisis. In Dobbs, the Supreme Court overturned the constitutionally protected right to access abortion, leaving the question of whether and how to regulate abortion to individual states. Approximately 22 million women and girls of reproductive age in the US now live in states where abortion access is heavily restricted, and often totally inaccessible. This briefing paper details the intensifying human rights emergency caused by the decision, and discusses the ways that Dobbs contravenes the US’ international human rights obligations.
The consequences of the Dobbs decision are wide ranging. Restrictions on access to healthcare places women’s lives and health at risk, leading to increased maternal mortality and morbidity, a climate of fear among healthcare providers, and reduced access to all forms of care. Dobbs also enables penalization and criminalization of healthcare, with providers, patients, and third parties at risk of prosecution or civil suit for their involvement in private healthcare decisions. Relatedly, the decision opens the door to widespread infringement of privacy rights as digital surveillance is expanded to detect violations of new regulations. New bans also infringe on freedom of thought, conscience and religion or belief, restricting the ability of physicians to counsel patients and clergy to provide pastoral care to their congregants. Finally, the harms of Dobbs violate principles of equality and non-discrimination; they fall disproportionately on marginalized populations including Black, indigenous, and people of color; people with disabilities; immigrants; and those living in poverty.
By overturning the established constitutional protection for access to abortion and through the passage of restrictive state laws, the US is in violation of its obligations under international law, codified in a number of human rights treaties to which it is a party or a signatory. These human rights obligations include, but are not limited to, the rights to: life; health; privacy; liberty and security of person; to be free from torture and other cruel, inhuman, or degrading treatment or punishment; freedom of thought, conscience, and religion or belief; equality and non-discrimination; and to seek, receive, and impart information.
A version of this briefing paper was submitted to UN special procedures mandate holders in March 2023. The submission, cosigned by nearly 200 human rights, reproductive justice, and other concerned groups and individuals, requested urgent action from the UN mandate holders to examine the situation, engage with civil society, and call on the US to uphold its international human rights obligations.
Less than a year on from this catastrophic legal decision, it is now apparent that the consequences are even worse than feared. Women and girls in need of reproductive healthcare are being met with systematic refusals, onerous financial burdens, stigma, fear of violence, and criminalization. Thousands are being forced to remain pregnant against their will.
Part II of this briefing paper outlines the consequences of Dobbs on the fundamental human rights of women and girls, as well as the disproportionate impact it has on certain demographics made vulnerable by systemic oppressions. This factual summary includes input from physicians in various states as part of fact-gathering efforts conducted by a number of organizations involved in this submission. Part III discusses the ways in which Dobbs contravenes the US’ international obligations. Part IV sets forth our Conclusion and Calls to Action.
II. Factual Background
- In June 2022, the US Supreme Court overturned the constitutionally protected right to access abortion,[2] leaving the question of whether and how to regulate abortion to individual states.[3] As of January 17, 2023, abortion is banned, with extremely limited exceptions, in thirteen states: Alabama, Arkansas, Idaho, Kentucky, Louisiana, Mississippi, Missouri, Oklahoma, South Dakota, Tennessee, Texas, West Virginia, Wisconsin, and Oklahoma.[4] Georgia has banned abortion after six weeks of pregnancy (effectively outlawing access entirely).[5] Approximately 22 million women and girls of reproductive age (ages 15-49) in the US live in states where abortion access is heavily restricted, and often totally inaccessible.[6] Four states have begun restricting access to medication abortions, including by prohibiting the mailing of medication into their jurisdictions.[7] Meanwhile, at least three states (Texas, Oklahoma, and Idaho) enacted so-called “bounty” laws before the Dobbs decision, empowering private citizens to sue providers who carry out abortions.[8] In continuation of the country’s devaluation of the lives of Black and Brown women, communities of color and of lower socio-economic status are bearing the brunt of these laws.[9] Dozens of clinics have closed across the country since Dobbs was decided,[10] increasing travel time and distance for women seeking care — and barring access for those women unable to travel.[11]
A. Women's Lives and Health on the Line
- The onslaught of legislative abortion restrictions in the US denies women’s decisional and bodily autonomy in a way that rejects the agency, dignity, and equality of people who can become pregnant.[12] This draconian attack on gender equality threatens women’s lives and health on a massive scale.
- In the months since Dobbs, two of the organizations involved in this submission have interviewed US healthcare practitioners about the impacts of anti-abortion legislation on women’s healthcare.[13] The practitioners’ responses describe far-reaching implications for women and girls seeking abortion and other reproductive healthcare, dramatically affecting their health, and resulting in serious — sometimes fatal — risks.
- These interviews and documentation by women’s rights groups describe difficulty, including:
- in accessing abortion in cases of miscarriage;
- forced travel across state lines in emergencies;
- denial of care in cases of ectopic pregnancy;
- hospitals delaying care until the woman’s health has deteriorated to a level most certainly to fit within narrow and vague “risk to life of the mother” exceptions;
- professionals withholding information fearing that their advice could violate anti-abortion laws;
- reduced access to non-reproductive healthcare (e.g. chemotherapy);
- the infliction of serious psychological harm on women and girls forced to carry an unwanted pregnancy;
- complications for adolescents forced to give birth;
- reduced access to other forms of reproductive healthcare including contraception;
- heightened risk of violence faced by pregnant individuals in abusive relationships; and
- pregnant individuals forgoing prenatal care to avoid surveillance.
- Anti-abortion legislation may also reduce access to reproductive healthcare in states where abortion is still legal, as patients are displaced from restrictive jurisdictions into already-overburdened clinics in jurisdictions where abortion remains legal.
- The accounts provided by the interviewed professionals are shocking. Dr. Lisa Harris, Professor of Obstetrics and Gynecology at University of Michigan Medical School, described how a patient treated at her institution for ectopic pregnancy — a life-threatening condition in which an embryo implants outside of the uterus and therefore cannot result in a healthy pregnancy and requires an abortion — had to travel from her home state, Ohio, to Michigan because she could not find a doctor willing to treat her in Ohio after their six-week abortion ban came into effect in June 2022.[14] More broadly, Dr. Harris commented that, in the six months between the overturn of Roe v. Wade (Roe)[15] and the passage of Michigan’s constitutional amendment protecting abortion access, some faculty and trainees with whom she works decided not to provide abortion care because of the potential risk of prosecution should Michigan’s 1931 abortion ban come into effect.[16]
- Dr. Elissa Serapio, an obstetrics and gynecology specialist (or OB-GYN, a doctor who specializes in pregnancy and female reproductive health), worked in Texas in the aftermath of the state’s six-week abortion ban in 2021. Dr. Serapio explained that her colleagues were forced to watch their patients’ health deteriorate before providing abortions due to the narrow exceptions for legal abortion where the “life of the mother” is at risk.[17] This challenge, Dr. Serapio noted, applied even when there was a zero percent chance that the pregnancy in question could result in a live birth.[18]
- Dr. Eleanor Drey, Medical Director of the Women’s Options Center and the Family Birth Center at San Francisco General Hospital, explained that physicians in states with abortion bans are now faced with two bad options: leave their patients to suffer harm or else risk prosecution.[19]
- While the array of state level abortion bans ostensibly have “exceptions” to safeguard the life and/or health of the pregnant person, these exceptions are unworkable. Replete with vague and non-medical terminology, the “exceptions” to protect women’s health and lives may be difficult to implement in practice, because their terms do not necessarily correspond with medical diagnoses and sometimes exclude health-threatening conditions.[20] Medical professionals report that the restrictive legal landscape means that they are generally unsure whether and when medically necessary, and even lifesaving, abortions are legal. They note that such uncertainty causes both healthcare providers and institutions to delay or deny abortion and other reproductive healthcare.[21] These dangerous chilling effects were foreseeable: research from other countries has long demonstrated the chronic unworkability, and concurrent danger, of general abortion prohibitions with exceptions to “save the life of the mother” or for “medical emergencies only.”[22]
- Several women who have been denied care in this way have bravely shared their experiences publicly. In July 2022, a woman had to travel hundreds of miles to a different state for a lifesaving abortion. Though she was experiencing an ectopic pregnancy (one of the leading causes of maternal mortality in the first 12 weeks of pregnancy)[23] her doctor would not end the pregnancy because he was “worried that the presence of a fetal heartbeat meant treating her might run afoul of new restrictions on abortion.”[24]
- In Wisconsin, hospital staff would not remove the fetal tissue for a patient with an incomplete miscarriage for fear that it would violate that state’s abortion ban.[25] She was left to bleed at home for more than 10 days.[26] While the patient survived and expelled the tissue safely, delays in miscarriage care — now common in anti-abortion states — pose serious risks to women’s health. Delays in expelling tissue following miscarriage can lead to hemorrhaging and life-threatening sepsis,[27] and can potentially impact future fertility.[28] Delayed care can also cause serious psychological suffering and trauma for women and families already dealing with pregnancy loss.[29]
- Moreover, risk-averse hospitals often fail to give healthcare teams the information they need to feel comfortable making such a medical decision. In Dr. Serapio’s experience, hospitals leave medical teams to make these decisions — and assume the risk that goes with them — alone.[32]
- The chilling effect of anti-abortion legislation may also cause physicians to withhold information from patients for fear that their medical advice could violate their state’s anti-abortion statutes.[33] Doctors report that the rapidly shifting landscape has impacted their ability to counsel patients, including full information on dealing with pregnancy complications and options for patients from across state lines: “We’re trying to be very, very careful,” said Dr. Katie McHugh, in an interview with National Public Radio (NPR), “And it is so scary to me to know that I'm not only worrying about my patients' medical safety, which I always worry about, but now I am worrying about their legal safety, my own legal safety. The criminalization of both patients and providers is incredibly disruptive to just normal patient care.”[34]
- Dr. Jennifer Griggs, a Professor in the University of Michigan’s Department of Internal Medicine, Hematology & Oncology Division, also spoke to the impact of abortion restrictions on women’s access to healthcare more broadly — even non-reproductive care.[35] She described how the legal landscape post-Dobbs leaves pregnant people and their clinicians in an untenable situation, risking the life of a pregnant patient by delaying treatment for a range of health conditions.[36] For example, she reported that anti-abortion laws challenge doctors’ ability to provide cancer treatment in a timely manner. Because treatments such as chemotherapy and radiation can harm a fetus, particularly during early pregnancy, laws that restrict women’s termination options can force them to delay cancer treatments until later in pregnancy when the risks are lowered or until they have given birth. Such delays, however, can put the patient’s life at risk.[37] The uncertainty of the law under state abortion bans also has what Dr. Harris refers to as a “coercive negative impact on patients,” in which concerns about restrictive or uncertain abortion regulations lead doctors or patients to make suboptimal decisions about a patient’s course of treatment.[38]
- Girls and adolescents are at increased risk of life-threatening consequences owing to delayed reproductive healthcare. Because girls and adolescents experience serious pregnancy-related complications at a higher rate than adults,[39] including, trauma to organs,[40] pregnant adolescents are particularly at risk when healthcare providers delay care. Despite this heightened vulnerability, none of the state abortion bans recognize an exception specifically for adolescent pregnancy.[41] Even before Dobbs, young people under 18 in at least 36 states faced “parental involvement” requirements forcing them to notify and/or seek permission from a parent to get an abortion. These restrictions remain in place in more than 20 states where abortion is still legal.[42] While most young people who have abortions voluntarily involve at least one parent in their decision, forced parental involvement laws put young people’s health and safety at risk. Young people without a supportive parent to involve in their abortion decision — for example, those who “fear physical or emotional abuse, being kicked out of the home, alienation from their families or other deterioration of family relationships or being forced to continue a pregnancy against their will”[43] — generally have the option to go through a judicial bypass process to request permission from a judge to access abortion care. However, the process for securing a bypass is daunting and unworkable for many young people.[44] A recent study by Human Rights Watch revealed that Florida judges denied more than one in eight young people's petitions in 2020-2021.[45] These children and adolescents were then forced to continue a pregnancy against their wishes, travel outside the state, or seek a way to manage abortion outside the health system.
- Abortion bans also harm women’s health in ways unrelated to pregnancy complications. Abortion restrictions can increase the risk of violence for pregnant individuals who are exposed to abusive relationships. Studies reveal that many victims of intimate partner or domestic violence seek abortions to prevent further abuse.[46] The inability to obtain an abortion can force victims to remain with their abusers.[47] These impacts are compounded for women from marginalized groups, who are more likely to experience domestic violence[48] and are less likely to have access to an abortion if the procedure has been banned in their state.
- Abortion bans can also increase the risk of suicide. Medical exceptions to abortion bans in the US do not provide for psychological risks to life or health.[49] This limitation prevents physicians from providing abortion care even if they have a well-founded fear that their patient will attempt suicide if forced to continue their pregnancy.[50] Federal guidance regarding the provision of emergency medical care does not explicitly mention mental health under emergency medical conditions that may require abortion.[51] In Dr. Drey’s experience, suicide risk is especially pronounced in some of her teenage patients who develop “post-traumatic stress disorder or suicidal ideation as a result of their pregnancies and make plans to commit suicide if they cannot obtain an abortion.”[52] For individuals who have become pregnant as a result of rape, this risk can also be heightened, Dr. Drey explained.[53]
- Even more starkly, pregnant people who attempt suicide can be charged with attempted feticide, manslaughter, or murder in some states.[54] For example, in 2011 in Indiana, Bei Bei Shuai, an immigrant woman from China, attempted suicide and was subsequently charged with murder and feticide for attempting suicide while pregnant, based on the prosecutor’s interpretation of the murder code to include fetuses.[55] As the zeal for prosecuting pregnant individuals increases,[56] there is a significant risk that abortion bans with fetal personhood language can use a pregnant person’s need for mental health support as a reason to funnel them into the criminal-legal system whilst simultaneously failing to address the underlying health issue.
- Abortion bans also reduce the quality and availability of other forms of necessary reproductive healthcare, such as contraception, pre- and postnatal care, and preventative annual exams.[57] One reason for this is that the reproductive healthcare clinics that provide this treatment are often financially unable to stay open when abortion services become illegal.[58] Some communities are facing reductions in care because their obstetricians have moved or are considering moving to states where abortion is still legal.[59]
- Even obstetric training is being impacted. Medical schools in anti-abortion states are limited in what they can teach about abortion, and young doctors are choosing to study — and eventually practice — elsewhere.[60] A research study mapping US residency programs predicted that almost 44% of OB-GYN residency programs are located in states that have already banned or are likely to ban abortions.[61] As more states ban or limit abortion, medical students may prefer to train in states where abortion is legal. Consequently, existing divides in healthcare access will deepen as many medical residents choose to practice where they trained.[62]
- Anti-abortion legislation also has a chilling effect on patients’ access to healthcare services more broadly. Access to healthcare in the US depends in part on access to insurance, and for many low-income individuals, the most available insurance provider is the federal government-run Medicaid system. Enrollment in Medicaid is limited by income level, but income caps for the program are higher for pregnant and postpartum individuals.[63] As a result, many low- and middle-income patients who have otherwise been excluded become eligible for the first time when they become pregnant.[64] This increased access to healthcare includes coverage for pre- and postnatal care, but also for non-pregnancy-specific care such as health screenings, hospital visits, and emergency care.[65] This window of increased access thus provides an opportunity for patients to be screened for a host of conditions.
- But criminalization of certain pregnancy outcomes discourages engagement with the healthcare system, leading to reduced prenatal care and worse health outcomes for pregnant people and infants alike. For example, the number of women receiving any prenatal care markedly dropped in Tennessee while the state’s law criminalizing any prenatal drug use was in effect, as pregnant people were threatened with criminal prosecution for a host of pregnancy outcomes and therefore avoided contact with formal healthcare.[66] The reduction in access was more pronounced for populations marginalized along class lines[67] and was associated with measurably worse health outcomes for mothers, fetuses, and newborns.[68] New abortion bans and criminalization can be expected to instill fear in pregnant patients[69] and create confusion over potential criminal liability, further reducing access to healthcare for vulnerable populations while increasing punitive surveillance of marginalized women.[70] Pregnant people — even those who wish to continue their pregnancies — may forgo prenatal care to which they are entitled altogether to avoid falling under surveillance.
- Abortion access is also threatened in states where abortion is still legal. Due to the rapidly changing legal landscape and fears of future legal consequences, some providers feel forced to suspend services even where abortion has not yet been outlawed. For instance, in West Virginia, the only abortion clinic in the state stopped performing abortions shortly after Dobbs was decided, even though the state’s pre-Roe abortion ban had not fully entered into force.[71] In Arizona, where a legislative attempt to ban abortion has been blocked by the courts, nine of the state’s ten clinics have nevertheless stopped providing abortions.[72] A provider in Arizona reported that she had decided to suspend abortion services because, as a Black doctor, she felt particularly vulnerable to potential criminalization. She noted “abortion is still legal but that would not stop someone from causing a legal disaster that I would not be able to recover from.”[73] Providers are hesitant to move to or continue practicing in states where restrictions are increasing or unstable, citing “an atmosphere … perceived as antagonistic to physicians.”[74] This dynamic deepens existing shortages of physicians, nurses, and other skilled providers.
- The chaos has spilled over to states where abortion is expected to remain legal. As patients are displaced from their home states by abortion prohibitions, providers in states where abortion remains legal are seeing an influx of patients, placing a large strain on already overtaxed clinics.[75] Clinics in less restrictive states often do not have enough staff. As Dr. Serapio explained, it can be difficult to find qualified staff because of the need for specialized training and experience.[76] Given the legal landscape over the past few years, obtaining the requisite formal and practical experience is difficult, so qualified staff was already in short supply.[77]
- Abortion providers also suffer risk to their physical safety and lives in the US. Both in their clinics and in their homes, many providers and other staff report being in near constant fear of attack from extremists within the anti-abortion movement.[78] Extremist anti-abortion vigilantes have kidnapped, attacked, bombed, and even murdered abortion providers.[79] In 2021 alone, the National Abortion Federation reported 1,465 incidents of violence against providers across the US.[80] The widespread organized campaigns of harassment and violence appear to have been emboldened in recent years by the movement’s broader success in restricting abortion.[81] Notably, those who target providers and clinic workers and harass abortion seekers often have ties to violent extremist movements. For instance, a number of violent anti-abortion extremists were documented at the January 6, 2021 coup attempt at the US Capitol.[82] As recently as January 15, 2023, an anti-abortion group carried out an arson attack on a clinic in Illinois.[83]
B. Penalizing Healthcare: Criminalization, Civil Liability, and Involuntary Confinement
- Following Dobbs, 13 states’ statutes now criminalize healthcare providers who perform abortions.[84] Penalties include up to life in prison (Texas)[85] and fines as much as $100,000 (Oklahoma).[86] Some states also impose criminal liability for “aiding or abetting” abortion, making it a crime for any individual, whether a healthcare provider or not, to assist a pregnant person in obtaining an abortion.[87] This can apply to hospital administrative staff, therapists, and other medical professionals who have discussed or provided information about obtaining an abortion; family, friends, or religious leaders; or even rideshare or cab drivers who transport patients to abortion clinics.[88] Employers, family members or friends who contribute financially or provide other forms of support can also be criminalized.[89]
- Individuals can also face civil penalties for “aiding and abetting” abortion in some states. Texas, for example, provides for privately enforced civil liability,[90] in addition to its criminal ban.[91] This threat of private suits places further pressure on providers to cease providing any abortion care whatsoever — even for patients who experience complications making abortion medically necessary and permitted under the state’s criminal restrictions — because they may have to defend themselves from a costly lawsuit brought by a bystander.[92] As Dr. Serapio explained, the law has left providers in Texas feeling potentially surveilled by everyone around them and questioning whether private discussions with their patients could land them in front of a judge.[93]
- Some states are attempting to enforce their bans across state lines. Although the legality of this strategy is uncertain,[94] lawmakers in several states that have banned abortion have proposed legislation to “allow private citizens to sue anyone who helps a resident of that state… terminate a pregnancy outside the state,” from an out-of-state physician who performs a procedure to a driver who conveys a patient across state lines.[95] For example, Missouri lawmakers introduced a bill in 2021 that claimed jurisdiction over any pregnancy conceived within the state or where the parents were Missouri residents.[96] While the law was not adopted, another bill introduced last year is intended to allow private enforcement across state lines.[97] These cross-border efforts expand the threat of prosecution beyond providers practicing in restrictive states, creating uncertainty for providers[98] even in states where abortions remain legal, and infringing on women’s freedom of movement.
- Pregnant individuals themselves are also at risk of criminalization.[99] In some states, officials have indicated a willingness to arrest those who self-induce abortion.[100] In Idaho, a statute from 1973 remains a potential threat: a woman “who purposely terminates her own pregnancy otherwise than by a live birth” can be found guilty of a felony.[101] Similarly, some states have begun to explore criminalization approaches based on “fetal personhood,”[102] a concept which attributes legal rights to a fetus.[103] If adopted, these provisions will increase prosecutions targeting pregnant people by classifying abortion as homicide and permitting prosecution of those who receive such treatment for murder or manslaughter.[104] A Louisiana House of Representatives committee voted in May 2022 to amend criminal laws to make abortion qualify as a homicide.[105] While the bill was subsequently withdrawn, other states are exploring fetal personhood approaches to criminalizing a range of pregnancy outcomes.[106]
- Even prior to Dobbs, prosecutors charged pregnant women and girls in situations where they suspected that the woman’s actions during pregnancy harmed the fetus.[107] Alleged conduct deemed worthy of prosecution went beyond suspected abortions to include using drugs (even where prescribed by a doctor), drinking alcohol, and falling down stairs.[108] For example, in 2020, a pregnant woman from Alabama was prosecuted for using pain medication prescribed by her doctor, even though it was established after the baby was born that the child suffered no adverse consequences.[109] In 2014, a pregnant woman who took just half a Valium pill and whose child was born healthy was charged with “chemical endangerment of a child.”[110] Pregnancy Justice, one of the organizations involved in preparing this submission, has documented more than 1700 instances of arrests, forced medical interventions, and other deprivations of liberty of pregnant people since 1973, with 1331 of these cases occurring between 2006-2020.[111] This sharp escalation in arrests engenders significant concern given that states now have no restrictions on their ability to criminalize women for their reproductive outcomes.
- Some jurisdictions also have policies of civil or administrative detention to hold pregnant girls and women in custody — even without criminal charges — if they are suspected of using controlled substances during pregnancy.[112] Thus even in states that do not explicitly criminalize women who seek abortions, authorities have used civil commitment and involuntary substance abuse treatment to detain individuals for allegedly endangering their fetuses.[113] Following their 2016 country visit to the US, the UN Working Group on arbitrary detention observed, “The civil proceedings to commit pregnant women are often in closed hearings, lack meaningful standards and provide few procedural protections. In some states, important early hearings may take place without the mother having legal representation, as the pregnant woman does not have the right to appointed counsel although the fetus has a court-appointed guardian ad litem.”[114] Pregnant individuals have been arbitrarily detained under these policies for months at a time. Because spontaneous miscarriage and self-managed abortion are medically indistinguishable in most cases,[115] prohibitions on abortion will predictably lead to the investigation and detention of many women experiencing miscarriages as well as those self-managing abortions.
- Those targeted for detention and criminalization are more likely to be Black, Indigenous, and people of color (BIPOC) individuals,[116] contributing to the already disproportionately high level of incarceration of BIPOC persons in the US.[117] For example, out of 413 cases of arrest or forced intervention of pregnant persons documented between 1973 and 2005, 71% were economically disadvantaged women, 59% were women of color, and 52% were Black.[118] Communities of color, especially Black communities, are disproportionately impacted by pregnancy criminalization due in part to the heightened policing of these communities under the auspices of the “war on drugs.”[119] As the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health has already described, “given that the country’s criminal legal system already disproportionately polices women and girls of African descent, [this] is the population group that suffers the most from increased surveillance and criminalization.”[120]
- Finally, the criminalization of abortion threatens to further affect the relationship between patients and their healthcare providers. Providers fear that their actions, or even their words, could be used against them in court. Patients may be afraid to seek care[121] and worry that providers will act as an arm of the police by collecting evidence and reporting them to the authorities if they suspect an abortion has been induced.[122] Since BIPOC individuals already face well-documented barriers to obtaining proper medical treatment and are subject to over-policing,[123] they are put at particular risk.[124]
- The ultimate impacts of abortion criminalization have not yet been fully realized, but it is reasonable to expect this criminalization to have a chilling effect on women’s health generally, to increase risks to women’s lives, and to lead to further arbitrary detention of women and girls.
C. Threats to Privacy from Increased Digital Surveillance
- The proliferation of abortion bans in the US has decimated reproductive autonomy — the power to control all aspects of one’s reproductive health — which is “at the very core of [individuals’] fundamental right[s] to equality and privacy.”[125] The right to privacy of individuals (irrespective of whether or not they are pregnant) and the rights of medical professionals are also threatened by states’ use of digital surveillance to track the identities of people who seek or provide reproductive healthcare.
- Because many states now criminalize abortion, law enforcement officials in these states are using electronic data to prosecute patients or those who help them access abortion.[126] This personal information is wide in scope and may include:
- location data to show if someone visited an abortion clinic, substance use disorder treatment center, or other health facility;
- search histories on medication abortion, clinics, and general information on abortion;
- menstrual cycle tracking applications; and
- communications data such as text messages about pregnancy and abortion.[127]
- The pre-Dobbs case of Latice Fisher, who was charged with second-degree murder after a stillbirth when investigators found the words “mifepristone” and “misoprostol” in her phone’s search history, shows how these tactics were used even while Roe was still in force.[128] Now that abortion is explicitly criminalized in many states, law enforcement’s use of digital surveillance to track abortions is likely to increase.
- Notably, law enforcement can access many of these sensitive personal records without a warrant. The legal standards for accessing novel digital evidence like location data vary depending on whether the data are obtained directly from the suspect (as in a search of a person’s cell phone), via an order issued to a third party (e.g. warrants issued to Google or Meta), or through purchases from data brokers[129] (i.e. individuals or companies that collect and aggregate many types of personal information usually from online sources).[130] This means that many of the usual limitations on police searches designed to protect defendants and prevent overbroad surveillance do not apply to all law enforcement access to personal information.[131]
- Purchasing data from brokers provides particularly easy and so-far unregulated law enforcement access to an unprecedented volume of sensitive personal information for use in prosecuting individuals seeking abortions — or even reviewing their options for reproductive care — often without any oversight by courts.[132]
- As with most aspects of abortion bans, these surveillance tactics will disproportionately affect marginalized individuals. BIPOC women, particularly Black women, are more likely to suffer miscarriages,[133] which are generally indistinguishable from medically induced abortions.[134] Combined with existing higher law enforcement surveillance rates of these communities,[135] these factors mean that BIPOC women will face higher rates of privacy infringement. Additionally, low-income women face surveillance and privacy intrusions not only from the government as a result of receiving government benefits, but also from employers monitoring workplace conduct and performance.[136] They also face financial barriers to protecting their privacy.[137] As a result, the privacy of BIPOC, low-income, and otherwise marginalized women will be violated disproportionately.
- Private parties including anti-abortion activists also use technology to gather data on both providers and pregnant people. For instance, anti-abortion groups have used mobile geo-fencing technology to target patients at abortion clinics with anti-abortion advertisements.[138] Anti-abortion centers known as “crisis pregnancy centers” and “abortion alternatives” hotlines also collect data on pregnant individuals.[139] In states such as Texas, which offer a bounty for citizens to bring civil lawsuits against anyone aiding and abetting an abortion, private parties may have a particular incentive to purchase abortion-related data. In May 2022, journalists revealed that they were able to purchase location data of individuals who visited Planned Parenthood centers for just $160 from a data broker — in the context of possible $10,000 bounties under the Texas law.[140] The purchased data are purportedly “anonymized,” but due to the small number of devices visiting these locations, it is often possible to de-anonymize the data (i.e. link to specific individuals).[141] These practices are emerging and evolving in a landscape without protections, as “the U.S. lack[s] a comprehensive set of federal digital privacy laws.”[142]
D. Freedom of Thought, Conscience and Religion or Belief
- Some forms of anti-abortion legislation in the US infringe upon the right to freedom of thought, conscience, and religion or belief under international human rights law. First, anti-abortion laws that prevent providers and/or clinic staff from providing abortions to pregnant persons may infringe upon the provider’s freedom to manifest their freedom of conscience and religion or belief. For some healthcare providers, their religion or beliefs (including non-theistic beliefs) mandate that they provide healthcare (including abortion) when a person’s life, health, or well-being is at risk. For example, Jewish physicians in Florida have explained in a lawsuit that their faith compels them to provide abortion to patients where the patient’s life, health or well-being is at risk.[143] For these and other healthcare workers, criminal abortion laws eviscerate their freedom to manifest a key aspect of their faith.[144]
- Even religious leaders and clergy members risk falling afoul of abortion laws in the US for providing pastoral care, guidance, and religious teaching. For faith leaders whose belief system affirms the right to abortion, counseling on reproductive healthcare in accordance with their faith could fall within the aforementioned broad crime of “aiding or abetting” an abortion. Members of the Unitarian Universalist Church in Florida have been forced to turn to the courts to seek injunctive relief against the law’s attempt to punish them for providing ministry and serving their congregants in this way.[145] Specifically, these clergy members underscore that counseling in line with their faith involves explaining the tenet of the “God-given right to self-determination over their own bodies and reproductive lives.”[146] But if a pregnant person has an abortion following a conversation on this area of the church’s doctrine, the clergy members could face prosecution for aiding, abetting, or encouraging abortion.
- Crucially, laws that criminally prosecute or otherwise punish people of faith who feel obligated by their religion or belief to help others access abortion, or to counsel congregants on abortion care, do not meet the thresholds set by international law that would permit the State to limit their freedom to practice their religion or belief. The right to manifest one’s religion or belief may be subject only to such “limitations as are prescribed by law and are necessary to protect public safety, order, health, or morals or the fundamental rights and freedoms of others.”[147]
E. Disproportionate Impact on Marginalized Populations
- Dobbs is devastating for all people who can become pregnant, but it has had and will have an outsized impact on certain marginalized groups who already face documented discrimination within and outside the healthcare system. This includes BIPOC women, people of diverse gender identities and sexual orientations, migrants, persons with disabilities, people who are low-income or living in poverty, children, and rural residents.[148] These groups often have poorer health outcomes compared to other populations,[149] and Dobbs will worsen these disparities, since individuals who belong to these groups have fewer resources and face discrimination from the healthcare community.[150]
- For people with disabilities, “[c]onstitutional protection for bodily autonomy is of vital importance… because that protection has far too often been denied to them in both reproductive and non-reproductive contexts.”[151] The Autistic Self Advocacy Network and the Disability Rights Education and Defense Fund note in their Dobbs amicus curiae brief that the US has a history of engaging in the forced sterilization of persons with disabilities, particularly targeting people of color with disabilities.[152] Individuals with disabilities have been continuously denied reproductive autonomy, and many fear the Dobbs decision will further entrench these policies and erode what progress they have achieved toward the protection of their bodily autonomy.[153]
- Communities marginalized by racial discrimination and oppression also face barriers in accessing healthcare, which severely and negatively impacts these communities. Indigenous Americans experience statistically worse healthcare outcomes than other populations in the US[154] and already had difficulty accessing abortion long before Dobbs.[155] The same is true for Black Americans, who have always faced high barriers to accessing healthcare.[156] Hence, individuals who belong to more than one marginalized group, such as rural Black Americans, face especially high barriers.[157] Access to abortion — and indeed to quality healthcare — has never been equitable for persons from marginalized communities in the US. Dobbs exacerbates many of these inequities by, for example, requiring individuals to travel farther for care and often out of state. Women of color are more likely to fall below the poverty line than white women and therefore feel the costs of interstate travel for healthcare particularly acutely. They are also less likely to have paid time off or paid sick leave to allow for travel, and face additional discrimination to obtain necessary healthcare.[158]
- Migrants and asylum seekers face further barriers in accessing reproductive healthcare.[159] Irregular immigration status prevents millions of individuals from qualifying for health insurance programs in general, and creates particular barriers to accessing insurance that covers reproductive healthcare services.[160] Immigrants also face mobility restrictions. Many US states require documentation of immigration status in order to receive a driver's license, and some of the most restrictive bans on abortion are in states (such as Texas) that host a network of Border Patrol checkpoints.[161] Undocumented immigrants who seek to cross state lines to access abortion care are at risk of arrest, detention, and deportation. As Dr. Serapio explained, for individuals who are undocumented and/or unauthorized, or who have undocumented and/or unauthorized family members, travel out of state is therefore not an option due to the possible legal ramifications, even where resources are available.[162]
- Youth with migrant status or with families that have mixed migration or documentation statuses face particular barriers in states where parental consent is required for abortion. For example, immigrant youth may lack access to a qualifying parent living in the country; immigrant parents may not be able to provide legally valid consent if they lack documentation of their legal status; and younger people with migrant status may be deterred from seeking healthcare or involving a parent by a general fear of immigration consequences for themselves or their families.[163] In these cases, immigrant youth may be forced to seek a judicial bypass or remain pregnant involuntarily.[164]
- State abortion bans have also led to the closure of reproductive health clinics that, in addition to abortion, provide non-abortion-related medical care upon which many individuals from vulnerable groups rely.[165] In general, the states enacting bans have some of the worst healthcare systems in the country and have historically dedicated few resources for low-income residents.[166] Lawmakers passing abortion bans have for years refused to address these problems.
- Rates of sexual violence against individuals in marginalized communities are also significantly higher than for the rest of the population.[167] Since many state laws prevent pregnant persons from obtaining an abortion even in circumstances of rape or incest,[168] these groups face an increased risk of being forced to continue a pregnancy that is the result of sexual violence. Even where a state has a legal exception allowing for abortions in cases of rape, these exceptions are extremely difficult for survivors to access in practice because they generally require filing an official police report before a provider can perform an abortion.[169] Given low rates of reporting of sexual violence, especially among marginalized communities including BIPOC and individuals of diverse gender identities and sexual orientations, these requirements effectively bar survivors from accessing abortion care.[170]
- Finally, Dobbs obliges many women to travel farther distances to obtain an abortion, due to state bans and clinic closures.[171] This means taking time off work, arranging childcare, and obtaining the funds to pay for travel expenses and accommodations.[172] Such laws have a disparate effect on persons of lower socio-economic status including those living in poverty. A pre-Dobbs study “found that the average travel distance to an abortion clinic [would] increase threefold — from nearly 40 to more than 113 miles — if the U.S. Supreme Court overturn[ed] Roe and restrictive state legislation kick[ed] in.”[173] This prediction has been borne out: early post-Dobbs analysis shows that travel time to clinics has increased significantly for people across the country.[174] Since individuals in marginalized groups are more likely to be low-income, this travel, and thus access to reproductive services, is often beyond their means.[175] A higher percentage of individuals from these marginalized communities will be unable to travel out of state for abortion and thus will be forced to bear a child for which they likely have fewer resources to provide.
- These barriers to access create a vicious cycle of poverty and marginalization, reinforcing existing inequalities. A study on abortion access – conducted before Dobbs was decided[176] – illustrates how abortion denial can reinforce economic and social marginalization. Based on thousands of interviews with women who sought, but were denied, an abortion, the study found that such patients are more likely to: (1) be exposed to significant health risks from delivery; (2) experience negative health outcomes over the next five years; (3) scale back their aspirations and career plans; (4) face long-term economic hardship; and (5) raise their children in poverty. In short, as the author of the study explained in a recent article, “we are about to see a deepening of existing inequalities…Being denied an abortion [will] lead[] to . . . greater poverty and health risks.”[177]
III. Anti-Abortion Legislation Violates International Law
IV. Conclusions and Calls to Action
The US has violated its human rights commitments by removing constitutional protection for reproductive healthcare. The Dobbs decision subjects all those who can become pregnant to barriers to medical care, criminalization and penalization, infringements on privacy and on freedom of conscience, with disproportionate impact on already-marginalized populations. Similarly, the multiplying restrictions on abortion expose healthcare practitioners, clergy, and others to criminalization, professional sanction, and infringements on privacy and on free exercise of thought, conscience and religious belief. These impacts contravene the US’s international treaty obligations to protect the rights to: life; health; privacy; liberty and security; freedom from torture or CIDT; freedom of thought, conscience, and religion or belief; equality and non-discrimination; and to seek, receive, and impart information.
In light of these violations, the US must take immediate steps to undo the grave harms caused by the Dobbs decision. The US should:
- By overturning the established constitutional protection for access to abortion, and through the passage of the state laws discussed above, the US is in violation of its obligations under international human rights law, codified in a number of human rights treaties to which it is a party or a signatory.
- Specifically, the US has ratified the International Covenant on Civil and Political Rights (ICCPR),[178] the International Convention on the Elimination of All Forms of Racial Discrimination (ICERD),[179] and the Convention Against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment (CAT).[180]
- The US also signed, but has not yet ratified, the International Covenant on Economic, Social and Cultural Rights (ICESCR),[181] the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW),[182] the Convention on the Rights of the Child (CRC),[183] and the Convention on the Rights of Persons with Disabilities (CRPD).[184] As a signatory to these treaties, the US must refrain from acts that would defeat their object and purpose.[185]
- These treaties enshrine in law numerous complementary human rights. The US has committed to respect and protect these rights; instead, it is infringing them through restrictions on abortion access. As eight Special Procedures mandate holders recently reaffirmed: “ Over time, States and human rights bodies clarified that human rights treaty obligations encompass the reproductive rights of women and girls, including safe and legal abortion access.”[186] These human rights obligations include, but are not limited to, the rights to: life; health; privacy; liberty and security of person; to be free from torture and other cruel, inhuman, or degrading treatment or punishment (CIDT); freedom of thought, conscience, and religion or belief; equality and non-discrimination; and to seek, receive, and impart information.[187]
- First, abortion laws and policies in the US endanger the life and health of persons seeking abortions and people in need of emergency reproductive healthcare. These policies contravene the US’ human rights obligations to respect the right to life[188] and the right to health.[189] As the Human Rights Committee (HRC) has confirmed, States parties to the ICCPR must not adopt anti-abortion measures that “result in violation of the right to life of a pregnant woman or girl” and must “provide safe, legal and effective access to abortion where the life and health of the pregnant woman or girl is at risk, or where carrying a pregnancy to term would cause the pregnant woman or girl substantial pain or suffering…”[190] States parties should also “remove existing barriers to effective access by women and girls to safe and legal abortion…and should not introduce new barriers.”[191] Other treaty bodies — including the Committee on Social, Economic and Cultural Rights (CESCR), the Committee on the Elimination of Discrimination against Women (CEDAW Committee), the Committee on the Rights of the Child (CRC Committee), the Committee on the Elimination of Racial Discrimination (CERD Committee), and the Committee on the Rights of Persons with Disabilities (CRPD Committee) — have unanimously and unambiguously recognized that access to abortion, and the ability to make free decisions regarding abortion, are indispensable to the fulfillment of the right to health.[192]
- In addition to the rights to life and health, abortion restrictions in the US also infringe the right to privacy[193] by allowing states to restrict reproductive choices and thereby to interfere with a pregnant individual’s physical and psychological integrity. HRC jurisprudence has firmly established that an individual’s decision to seek an abortion falls under the scope of the right to privacy.[194] The HRC has also found that some abortion bans, similar to those being enacted in the US, constitute impermissible interference with the ability to decide whether and how to proceed with a pregnancy, contrary to the right to privacy protected by Article 17 of the ICCPR.[195] Some US laws, particularly those imposing broad accessory liability on anyone who “advise[s] or encourage[s]”[196] a woman to get an abortion also infringe the freedom of a pregnant person to seek, receive, and impart information and ideas, guaranteed by Article 19 of the ICCPR.[197]
- Further, certain state laws, particularly those that criminalize abortion and/or provide no exception in the event of rape, incest, threat to the life or health of the pregnant person, or fatal fetal anomaly,[198] violate the right to be free from torture and other CIDT.[199] The Committee against Torture (CAT Committee) has acknowledged that abortion laws and denial of abortion can result in “physical and mental suffering so severe in pain and intensity as to amount to torture,”[200] a view echoed by the former Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment.[201]
- The CAT Committee has also affirmed that narrow exceptions only to save the life of the pregnant person, but not permitting abortions to preserve their health, are not sufficient to satisfy the requirement that States parties refrain from adopting policies amounting to torture or CIDT.[202] The HRC has likewise found that restrictions on access to abortion in cases of rape, incest, fetal anomaly, or to protect the life or health of the pregnant person violate the right to be free from torture and other CIDT under Article 7 of the ICCPR.[203] Notably, the HRC explicitly acknowledged that the right protected by Article 7 “relates not only to acts that cause physical pain but also to acts that cause mental suffering.”[204] The CEDAW Committee has also found that “criminalization of abortion, denial or delay of safe abortion and/or post-abortion care, [and] forced continuation of pregnancy... are forms of gender-based violence that... may amount to torture or cruel, inhuman or degrading treatment.”[205]
- The arrest and imprisonment of individuals on abortion-related charges — including those experiencing miscarriage or stillbirth — infringes upon the right to liberty and security of the person protected by Article 9 of the ICCPR.[206] The Special Rapporteur on health has explained the link between abortion restrictions and deprivations of the right to liberty: “Where abortion is illegal, women may face imprisonment for seeking an abortion and emergency services for pregnancy-related complications, including those due to miscarriages.”[207] In 2018, when reviewing El Salvador’s compliance with the ICCPR, the HRC specifically urged the State party to “suspend immediately the criminalization of women for the offence of abortion.” The HRC also urged the State party to “review all cases of women who have been imprisoned for abortion-related offences, with the aim of ensuring their release….”[208]
- Expanding the grounds for civil or administrative detention of pregnant individuals for the “protection” of the fetus[209] also violates the right to be free from arbitrary arrest or detention.[210] Observing the trend of civil confinement of pregnant individuals for suspected use of drugs following a country visit in 2016, the Working Group on arbitrary detention concluded that such civil confinement “lacks due process…” and concluded “[t]his form of deprivation of liberty is gendered and discriminatory in its reach and application, as pregnancy, combined with the presumption of drug or other substance abuse, is the determining factor for involuntary treatment.”[211]
- Abortion bans also infringe upon the right to freedom of thought, conscience, and religion or belief, specifically the freedom to manifest religion or belief.[212] Manifestation of religion or belief includes “worship, observance, practice and teaching.”[213] As the mandate of the UN Special Rapporteur on freedom of religion or belief has outlined, the right involves “not only the “believing,” but also the “belonging” and the “behaving” in line with one’s religion or belief.[214] This manifestation component of the right, also known as the forum externum, is not, however, unlimited. Article 18(3) of the ICCPR sets out the parameters of the State’s authority to limit the freedom to manifest a religion or belief, providing that the right “may be subject only to such limitations as are prescribed by law and are necessary to protect public safety, order, health, or morals[215] or the fundamental rights and freedoms of others.” Governments can apply these limits to freedom of religion or belief only for those purposes for which they were prescribed and the limits must be directly related and proportionate to the specific need on which they are predicated.[216] The HRC and the mandate of the UN Special Rapporteur on freedom of religion or belief have also clarified that restrictions may not be imposed for discriminatory purposes or applied in a discriminatory manner.[217]
- Restrictions on a rights-holder’s ability to behave in accordance with their religion or beliefs by providing abortion care do not conform to the limits set out in Article 18(3). First, these laws do not fall within the permitted exceptions because they are indeterminate. The HRC has explained that under the first criterion for limiting freedom of religion or belief, “law” must be “formulated with sufficient precision to enable an individual to regulate his or her conduct accordingly and it must be made accessible to the public.”[218] As described above, the myriad state laws that criminalize abortion provision and, in some states, “aiding or abetting” an abortion, are plagued by legal ambiguity.[219] As such, for the healthcare provider who is compelled to provide abortions because of their beliefs, the state’s efforts to limit their manifestation of their religion or belief is legally indeterminate, and therefore incompatible with Article 18(3).
- Second, the state’s limit on the manifestation of freedom of religion or belief is not sanctioned by international human rights law because it does not serve a legitimate aim under international human rights law. Rather than serve safety, order, health, morals, or the fundamental rights and freedoms of others, the abundance of criminal abortion laws that restrict rights-holders’ freedom of religion or belief endanger people’s lives and violate numerous fundamental human rights.[220] Thirdly, even if such limits on the right could be said to pursue a legitimate aim under Article 18(3), (which, we argue, they cannot) the extreme punitive measures for providing care could not be construed as proportionate. The HRC has clarified that governmental restrictions on a right must be the least restrictive among all the adequate measures that could be applied.[221]
- Restricting access to abortion discriminates against women and girls, breaching the right to equality and freedom from discrimination on the basis of gender.[222] In its communications to the State party in Mellet v. Ireland and Whelan v. Ireland, the HRC outlined the gender discriminatory nature of abortion criminalization, noting that Ireland’s criminal abortion law subjected women “to a gender-based stereotype of the reproductive role of women primarily as mothers” and that “stereotyping [a woman] as a reproductive instrument subjected her to discrimination.”[223]
- The CEDAW Committee has explicitly recognized the gender-discriminatory nature of abortion restrictions: “It is discriminatory for a State party to refuse to provide legally for the performance of certain reproductive health services for women.”[224] Elaborating on the discriminatory nature of the restrictive legal landscape for abortion in Northern Ireland in 2018, the CEDAW Committee further found, “that the failure to combat stereotypes depicting women primarily as mothers exacerbates discrimination against women and violates article 5, read with articles 1 and 2, of the Convention.”[225] Similarly, the UN Working Group on discrimination against women and girls (WGDAW) has emphasized that “the right to safe termination of pregnancy is an equality right for women.”[226]
- Restrictions on abortion can also violate the right to be free from racial discrimination. The CERD Committee has explicitly indicated that restrictions on abortion that disproportionately impact racial and ethnic minorities[227] run afoul of international obligations to eliminate racial discrimination.[228] In its 2022 review of the US, the CERD Committee expressed “deep[] concern[] at the Supreme Court’s ruling in Dobbs v. Jackson Women’s Health Organization, of 24 June 2022, which overturned nearly 50 years of protection of women’s access to safe and legal abortion in the State party; at the consequent profound disparate impact on the sexual and reproductive health and rights of racial and ethnic minorities, in particular, those with low incomes; and at the disparate impact of legislation and other measures at the state level restricting access to safe and legal abortion or criminalizing abortion.”[229] The Committee recommended that the US “take all measures necessary…to provide safe, legal and effective access to abortion in accordance with the State party’s international human rights obligations.”[230]
- Abortion restrictions can violate the right to be free from discrimination on the basis of socio-economic status or age as well. In Mellet v. Ireland, the HRC found that “the differential treatment to which [the woman seeking an abortion] was subjected in relation to other similarly situated women failed to adequately take into account her medical needs and socio-economic circumstances and did not meet the requirements of reasonableness, objectivity and legitimacy of purpose.”[231] Accordingly, the HRC concluded that the failure of Ireland “to provide services to [the woman] that she required constituted discrimination and violated her rights under article 26 of the Covenant.”[232] Similarly, the WGDAW observes, “in countries where induced termination of pregnancy is restricted by law and/or otherwise unavailable, safe termination of pregnancy is a privilege of the rich, while women with limited resources have little choice but to resort to unsafe providers and practices.”[233] The Working Group observed that abortion restrictions do not decrease overall abortion rates, but only rates of safe abortions, and concluded: “This results in severe discrimination against economically disadvantaged women.”[234]
- The CRC Committee has highlighted the discrimination faced by youth seeking abortions, finding that “particular efforts need to be made to overcome barriers of stigma and fear experienced by, for example, adolescent girls, girls with disabilities and lesbian, gay, bisexual, transgender and intersex adolescents, in gaining access to such services.”[235] The Committee also urged states to eliminate barriers, such as third-party consent or authorization requirements, that block adolescents and children from accessing abortion care, and recommended that states “decriminalize abortion to ensure that girls have access to safe abortion and post-abortion services, review legislation with a view to guaranteeing the best interests of pregnant adolescents and ensure that their views are always heard and respected in abortion-related decisions.”[236]
- Finally, some restrictions on abortion implicate the human rights obligations of private companies. Corporations have obligations to respect human rights, safeguard users’ rights to privacy, and ensure their services are not used in ways that cause or contribute to human rights violations.[237] This includes adopting policies that protect users from unwarranted government surveillance and harassment.[238]
- Against this backdrop, it is no surprise that the Dobbs decision was greeted with international condemnation. Then-UN High Commissioner for Human Rights Michelle Bachelet Jeria described the decision as a “setback after five decades of protection for sexual and reproductive health and rights…”[239] UN human rights experts representing diverse mandates concluded that Dobbs is “a shocking and dangerous rollback of human rights that will jeopardize women’s health and lives… [and it is] a monumental setback for the rule of law and for gender equality. With the stroke of a pen and without sound legal reasoning, the US Supreme Court has stripped women and girls in the United States of legal protections necessary to ensure their ability to live with dignity.”[240
- Enact a federal law that enshrines the right to abortion access as a human right in accordance with the 2022 World Health Organization Abortion Care Guidelines[241] and that preempts state laws restricting abortion.
- Take measures at the state and federal level to:
- Ensure the right to safe and legal abortion and reproductive healthcare;
- Ensure the right to seek information and consultation regarding birth control and pregnancy options;
- Require all health services to be provided in compliance with human rights standards;
- Ensure access to a full range of modern contraception, without discrimination or coercion;
- Remove all legal obstacles, including parental involvement laws, to accessing affordable, non-discriminatory, and quality comprehensive sexual and reproductive healthcare, including safe abortion;
- Protect the confidentiality of persons who can become pregnant and medical professionals by: (1) limiting the collection of patient data; (2) prohibiting the disclosure of confidential information to any third parties, including law enforcement, without consent; and (3) informing patients of their right to privacy and the confidentiality of their visit and queries;
- Protect medical professionals who provide abortion and other reproductive healthcare by prohibiting their prosecution, disbarment, loss of license, or other retribution or reprimanding measures;
- Fund medical facilities that provide access to abortion care and evidence-based, non-biased pregnancy and abortion-related information and counseling, especially in areas where minority and marginalized populations reside;
- Adopt a federal law that prohibits the criminalization of interstate travel for medical care, and assistance thereof;
- Address discrimination on the basis of disability throughout all aspects of reproductive healthcare;
- Address racial and ethnic origin discrimination in healthcare and health outcomes directly, through measures that: (1) remedy structural racism and intersectional discrimination; (2) make resources available to communities of color affected by reproductive health inequities; and (3) prioritize the meaningful participation and leadership of BIPOC people in all systems and at all points of decision-making processes that impact their reproductive health and rights.
As previously noted, a version of this briefing paper was submitted to UN special procedures mandate holders in March 2023. The submission requested urgent action from the UN mandate holders to examine the situation, engage with civil society, and call on the US to uphold its international human rights obligations.
The US has taken a dramatic step backwards in the protection of human rights by removing national safeguards for people who can become pregnant’s health, liberty, autonomy, privacy, and equality. The harms documented in the foregoing pages will only multiply as restrictions on essential healthcare increase.
[1] This paper refers interchangeably to “people who can become pregnant” and “women and girls” as the targets of laws restricting abortion. Although most people who can become pregnant and require abortion services are cisgender women, we recognize that people with diverse gender identities may also need abortions and are profoundly affected by abortion restrictions. For more information on the need for abortion services amongst trans, non-binary and gender diverse people in the United States, see H. Moseson et al., Abortion experiences and preferences of transgender, nonbinary, and gender-expansive people in the United States, 224 Am. J. Obstetrics & Gynecology 4 (2021); American College of Obstetricians and Gynecologists, ACOG Committee Opinion: Health Care for Transgender and Gender Diverse Individuals, 137 Obstetrics & Gynecology 3, p. e80-e81 (Mar. 2021), https://www.acog.org/-/media/project/acog/acogorg/clinical/files/committee-opinion/articles/2021/03/health-care-for-transgender-and-gender-diverse-individuals.pdf.
[2] Dobbs v. Jackson Women's Health Org., 142 S. Ct. 2228 (2022) (Dobbs v. JWHO).
[3] Id., p. 2243.
[4] Some states, such as Indiana and Ohio, have enacted bans that are currently under injunction as litigation moves forward. See “After Roe Fell: Abortion Laws By State,” Center for Reproductive Rights (updated in real time), https://reproductiverights.org/maps/abortion-laws-by-state/. In the November 2022 election, Kentucky voters rejected a ballot initiative to specify that the state constitution does not protect the right to abortion; however, the impact of the initiative is not yet clear, and Kentucky’s trigger ban is still in place. See A. Rickert, “Kentucky voters reject amendment that would have affirmed no right to abortion,” NPR (9 Nov. 2022), https://www.npr.org/2022/11/09/1134835022/kentucky-abortion-amendment-midterms-results. Other state bans have been blocked by courts: Arizona, North Dakota, Utah, and Wyoming. “Tracking the States Where Abortion is Now Banned,” The New York Times (updated 6 Jan. 2023), https://www.nytimes.com/interactive/2022/us/abortion-laws-roe-v-wade.html.
[5] See id. See also Center for Reproductive Rights, “After Roe Fell: Abortion Laws By State,” https://reproductiverights.org/maps/abortion-laws-by-state/. Ohio passed a similar six-week ban, but the provision has been blocked by a court and is currently on hold indefinitely. See “Tracking the States Where Abortion is Now Banned,” The New York Times (updated 6 Jan. 2023), https://www.nytimes.com/interactive/2022/us/abortion-laws-roe-v-wade.html.
[6] Guttmacher Institute, “100 Days Post-Roe: At Least 66 Clinics Across 15 US States Have Stopped Offering Abortion Care” (6 Oct. 2022), https://www.guttmacher.org/2022/10/100-days-post-roe-least-66-clinics-across-15-us-states-have-stopped-offering-abortion-care.
[7] Guttmacher Institute, State Legislation Tracker: Medication Abortion (updated 31 Dec. 2022) https://www.guttmacher.org/state-policy.
[8] Okla. Stat. tit. 63, §1-745.33-.34, .38 (2022); Idaho Code §§ 18-8804, 18-8807; Texas Heartbeat Act, Senate Bill 8 (SB 8) (20 Mar. 2021). See also S. Murphy, “Oklahoma Governor Signs the Nation’s Strictest Abortion Ban,” AP News (25 May 2022), https://apnews.com/article/abortion-us-supreme-court-health-texas-oklahoma-ad37e8db8a0f3fd9f4fcd215f8a3ed0a. These laws are still in effect post-Dobbs.
[9] See CERD Committee, Concluding observations on the combined tenth to twelfth reports of the United States of America (U.N. Doc. CERD/C/USA/CO/10-12) (21 Sept. 2022), ¶ 35. See also Global Justice Center, “United States of America: Submission to the United Nations Committee on the Elimination of Racial Discrimination,” pp. 11-12 https://www.hrw.org/sites/default/files/media_2022/07/SBRWI_HRW_GJC_AI_CERDShadowReport.pdf; Guttmacher Institute, “Inequity in US Abortion Rights and Access” (17 Jan. 2023), https://www.guttmacher.org/2023/01/inequity-us-abortion-rights-and-access-end-roe-deepening-existing-divides.
[10] Abortion Care Network, “Communities Need Clinics, The New Landscape of Independent Abortion Clinics in the United States” (2022 Report), https://abortioncarenetwork.org/wp-content/uploads/2022/12/communities-need-clinics-2022.pdf.
[11] Guttmacher Institute, “100 Days Post-Roe: At Least 66 Clinics Across 15 US States Have Stopped Offering Abortion Care” (6 Oct. 2022), https://www.guttmacher.org/2022/10/100-days-post-roe-least-66-clinics-across-15-us-states-have-stopped-offering-abortion-care.
[12] For more on the autonomy, dignity and equality impacts of abortion restrictions, see CEDAW Committee, Inquiry concerning the U.K. and Northern Ireland under article 8 of the Optional Protocol to CEDAW (U.N. Doc. CEDAW/C/OP.8/GBR/1, 17) (6 Mar. 2018) (“criminalization has a stigmatizing impact on women and deprives them of their privacy, self-determination and autonomy of decision, offending women’s equal status, constituting discrimination.”). See also Working Group on the issue of discrimination against women in law and in practice, Women’s Autonomy, Equality and Reproductive Health in International Human Rights: Between Recognition, Backlash and Regressive Trends (Oct. 2017) (“both the CEDAW Committee and the WGDAW determined that the right to safe termination of pregnancy is an equality right for women.”).
[13] Foley Hoag LLP, legal counsel to the Global Justice Center, interviewed medical professionals, including three OBGYNs (Drs. Harris, Serapio, and Drey), as well as a researcher who studies the impact of abortion on women (Dr. Foster). The methodology for these interviews included providing each interviewee with background on the purpose of the submission to the Mandate Holders and then asking about their general views about the change in laws as experienced by them, and their experience (before and after the change) performing abortions, treating patients who sought abortions, or otherwise treating patients. PHR engaged in a series of discussions with various medical sector stakeholders and clinicians post-Dobbs to understand the scope and nature of impacts of the decision on clinicians in the U.S., including specifically medical students through PHR’s Student Advisory Board.
[14] Interview by Foley Hoag LLP with Dr. Lisa Harris (4 Nov. 2022).
[15] Roe v. Wade, 410 U.S. 113, 153 (1973) (recognizing “the right of the woman to choose to have an abortion before viability”).
[16] Id. Dr. Harris also reported that many colleagues only feel comfortable providing abortion care in hospital settings, rather than clinics where abortion care is normally provided because they perceive the risk of prosecution to be lower in hospitals than in an outpatient setting. See Mich. Const. art. 1, § 28 (recognizing a fundamental individual right to reproductive freedom, including abortion care, adopted by ballot initiative Nov. 2022).
[17] Interview by Foley Hoag LLP with Dr. Elissa Serapio (29 July 2022).
[18] Id.
[19] Interview by Foley Hoag LLP with Dr. Eleanor Drey (15 July 2022).
[20] See e.g., E. Woodruff, “Louisiana hospital denies abortion for fetus without a skull” (17 Aug. 2022), https://www.nola.com/news/healthcare_hospitals/article_d08b59fe-1e39-11ed-a669-a3570eeed885.html. A Louisiana woman was denied an abortion in by a hospital after her fetus was diagnosed with acrania – developing without a skull – a condition considered “uniformly fatal in the perinatal period.” Because acrania did not appear on a state list of conditions considered to render a fetus “medically futile,” Louisiana doctors declined to perform the abortion, despite the physical and psychological health risks of continuing a pregnancy that will end in stillbirth or death within hours of birth.
[21] See generally Sens. Elizabeth Warren et al., Post-Roe Abortion Bans Threaten Women’s Lives: Health Care Providers Speak Out on the Devastating Harm Posed by Abortion Bans and Restrictions (Oct. 2022), https://www.warren.senate.gov/imo/media/doc/Abortion%20Care%20Oversight%20Report1.pdf. See also T. Weinberg, “Missouri doctors fear vague emergency exception to abortion ban puts patients at risk,” Missouri Independent (2 July 2022), https://missouriindependent.com/2022/07/02/missouri-doctors-fear-vague-emergency-exception-to-abortion-ban-puts-patients-at-risk/.
[22] For example, in the Dominican Republic, where abortion is criminalized, “[m]edical providers said that criminal penalties for abortion made it difficult for them to exercise their best judgment and provide the best standard of care when their pregnant patients faced serious health risks.” Human Rights Watch, “‘It’s Your Decision, It’s Your Life’ The Total Criminalization of Abortion in the Dominican Republic” (19 Nov. 2018), https://www.hrw.org/report/2018/11/19/its-your-decision-its-your-life/total-criminalization-abortion-dominican-republic. In Poland, where abortion is almost completely outlawed, pregnant women with cancer have been prevented from obtaining an abortion or otherwise accessing chemotherapy due to the potential harm to the fetus, placing more importance on the fetus than the pregnant person. See Human Rights Watch, “Regression on Abortion Harms Women in Poland” (26 Jan. 2022), https://www.hrw.org/news/2022/01/26/regression-abortion-harms-women-poland; Amnesty International, “Poland: A Year On, Abortion Ruling Harms Women” (19 Oct. 2021), https://www.amnesty.org/en/latest/news/2021/10/poland-a-year-on-abortion-ruling-harms-women/.
[23] See UC Davis Health, “7 things to know about ectopic pregnancy” (22 Mar. 2022), https://health.ucdavis.edu/news/headlines/7-things-to-know-about-ectopic-pregnancy/2022/05; J. Tenore, Ectopic Pregnancy, 61(4) Am Fam Physician 1080 (2000), https://www.aafp.org/pubs/afp/issues/2000/0215/p1080.html.
[24] F. Sellers & F. Nirappil, “Confusion post-Roe spurs delays, denials for some lifesaving pregnancy care,” The Washington Post (16 July 2022), https://www.washingtonpost.com/health/2022/07/16/abortion-miscarriage-ectopic-pregnancy-care.
[25] Id.
[26] Id.
[27] See P. Belluck, “They Had Miscarriages, and New Abortion Laws Obstructed Treatment,” The New York Times (17 July 2022), available at https://www.nytimes.com/2022/07/17/health/abortion-miscarriage-treatment.html. See also A. Redinger & H. Nguyen, Incomplete Abortions, StatPearls [Internet] (27 June 2022), https://www.ncbi.nlm.nih.gov/books/NBK559071/ (describing “complications that can arise after the management of incomplete abortion including death, uterine rupture, uterine perforation, subsequent hysterectomy, multisystem organ failure, pelvic infection, cervical damage, vomiting, diarrhea, infertility, and/or psychological effects.”).
[28] See generally A. Redinger & H. Nguyen, Incomplete Abortions, StatPearls [Internet] (27 June 2022), https://www.ncbi.nlm.nih.gov/books/NBK559071/ (describing “complications that can arise after the management of incomplete abortion including death, uterine rupture, uterine perforation, subsequent hysterectomy, multisystem organ failure, pelvic infection, cervical damage, vomiting, diarrhea, infertility, and/or psychological effects.”).
[29] See generally A. Redinger & H. Nguyen, Incomplete Abortions, StatPearls [Internet] (27 June 2022), https://www.ncbi.nlm.nih.gov/books/NBK559071/ (describing “complications that can arise after the management of incomplete abortion including death, uterine rupture, uterine perforation, subsequent hysterectomy, multisystem organ failure, pelvic infection, cervical damage, vomiting, diarrhea, infertility, and/or psychological effects.”). See also R. Westwood, “Bleeding and in pain, she couldn't get 2 Louisiana ERs to answer: Is it a miscarriage?” NPR (29 Dec. 2022), https://www.npr.org/sections/health-shots/2022/12/29/1143823727/bleeding-and-in-pain-she-couldnt-get-2-louisiana-ers-to-answer-is-it-a-miscarria.
[30] See e.g., Fla. Stat. § 390.0111 (1)(a) (requiring for any abortion after 15 weeks gestational age that "Two physicians certify in writing that, in reasonable medical judgment, the termination of the pregnancy is necessary to save the pregnant woman’s life or avert a serious risk of substantial and irreversible physical impairment of a major bodily function of the pregnant woman other than a psychological condition.”)
[31] Interview by Foley Hoag LLP with Dr. Elissa Serapio (29 July 2022).
[32] Id.
[33] J. Glenza, “A Severe Chilling Effect’: Abortion Bans Will Inhibit Doctors’ Advice to Patients, Experts Fear,” The Guardian (6 May 2022), https://www.theguardian.com/world/2022/may/06/abortion-bans-patient-doctor-medical-advice; (Noting the chilling effect of abortion bans among doctors counseling patients on options during pregnancy, including whether abortion care could be available in another jurisdiction).
[34] S. Simmons-Duffin, “Doctors Weren’t Considered in Dobbs, But Now They’re on Abortion’s Legal Front Lines,” NPR (3 July 2022), https://www.npr.org/sections/health-shots/2022/07/03/1109483662/doctors-werent-considered-in-Dobbs-but-now-theyre-on-abortions-legal-front-lines. For more on criminalization, see infra Section I(B).
[35] Interview by Physicians for Human Rights with Dr. Jennifer Griggs (22 Nov. 2022).
[36] Id.
[37] Id.
[38] Interview by Foley Hoag LLP with Dr. Lisa Harris (4 Nov. 2022). Dr. Harris described a patient pregnant with twins who experienced a complication requiring the termination of one fetus for the other to survive. This procedure should normally be completed after a certain stage of pregnancy to minimize the chance of complications or death. However, due to concerns over the shifting legal landscape, the patient elected to have the procedure earlier than medically advised. This decision – prompted by abortion bans and legal uncertainty – placed the health of the mother and the remaining fetus at risk.
[39] See World Health Organization, “Adolescent Pregnancy” (15 Sept. 2022), https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy; D. Jeha et. al., A review of the risks and consequences of adolescent pregnancy, 8 J. Neonatal-Perinatal Medicine (2015), pp. 1, 3.
[40] D. Jeha et. al., A review of the risks and consequences of adolescent pregnancy, 8 J. Neonatal-Perinatal Medicine (2015), p. 3.
[41] See supra note 9.
[42] Guttmacher Institute, “Parental Involvement in Minors’ Abortions,” (updated 1 Jan. 2023), https://www.guttmacher.org/state-policy/explore/parental-involvement-minors-abortions.
[43] In some states with parental notification requirements, there are provisions for judicial bypass of the requirement; however, the process for securing a bypass is daunting and unworkable for many girls and adolescents, requiring them to demonstrate that they are “1) sufficiently mature and well enough informed to make an abortion decision without parental involvement, and/or that 2) parental involvement is not in their best interests.” Perversely, these requirements can result in a judicial finding that a minor is “not sufficiently mature” to make an informed abortion decision, therefore forcing the child to remain pregnant and give birth. See, e.g., Human Rights Watch, “The Only People It Really Affects Are the People It Hurts” (11 Mar. 2021), https://www.hrw.org/report/2021/03/11/only-people-it-really-affects-are-people-it-hurts/human-rights-consequences.
[44] Id. In most states, to obtain a judicial waiver, young people must demonstrate that they have sufficient maturity to have an abortion without parental involvement, or that parental involvement is not in their best interest. Perversely, these requirements can result in a judicial finding that a minor is “not sufficiently mature” to make an informed abortion decision, therefore forcing the child to remain pregnant and potentially give birth.
[45] Human Rights Watch, “Access Denied: How Florida Judges Obstruct Young People’s Ability to Obtain Abortion Care” (19 Feb. 2023), https://www.hrw.org/news/2023/02/09/us-florida-judges-block-youth-abortion-access
[46] S. Roberts et al., Risk of violence from the man involved in the pregnancy after receiving or being denied an abortion, 12 Cent BMC Medicine 144 (2014) (explaining that women denied an abortion remain tethered to abusive partners and at risk for continued violence, even if they leave the relationship).
[47] Id.
[48] See Center for Disease Control and Prevention, Violence Against Native Peoples Fact Sheet (2020), https://www.cdc.gov/injury/pdfs/tribal/Violence-Against-Native-Peoples-Fact-Sheet.pdf (estimating that 48% of American Indian and Alaskan Native women will experience sexual violence, physical violence, and/or stalking from an intimate partner) (citing The National Intimate Partner and Sexual Violence Survey, Center for Disease Control and Prevention, Violence Prevention (updated 19 July 2021), https://www.cdc.gov/violenceprevention/datasources/nisvs/index.html); Women of Color Network, “Life in the Margins: Expanding Intimate Partner Violence Services for Women of Color by Using Data as Evidence” (June 2017), https://vawnet.org/material/life-marginsexpanding-intimate-partner-violence-services-women-color-using-data-evidence (showing that “[a]pproximately four out of every ten non-Hispanic Black women . . . have been the victim of rape, physical violence, and/or stalking by an intimate partner in their lifetime”).
[49] Of the statutes banning abortion in the US, none include exceptions to protect a pregnant person’s mental health. Some specifically exclude physical harms related to psychological distress. For example, Idaho’s law explicitly states that “No abortion shall be deemed necessary to prevent the death of the pregnant woman because the physician believes that the woman may or will take action to harm herself” (Idaho Code § 18-622(1)(a)).
[50] Interview by Foley Hoag LLP with Dr. Eleanor Drey (15 July 2022).
[51] See U.S. Dept. of Health and Human Services, Reinforcement of EMTALA Obligations specific to Patients who are Pregnant or are Experiencing Pregnancy Loss (11 July 2022), https://www.cms.gov/files/document/qso-22-22-hospitals.pdf. See also U.S. Dept. of Health and Human Services, Letter to U.S. Governors on Reproductive Health Care (26 Aug. 2022), https://www.hhs.gov/sites/default/files/hhs-letter-to-governors-reproductive-health-care.pdf.
[52] Interview by Foley Hoag LLP with Dr. Eleanor Drey (15 July 2022). Dr. Drey reported treating a pediatric patient whose pregnancy was caused by rape, who experienced post-traumatic stress disorder symptoms every time the fetus moved and was at risk of suicide as a result.
[53] Evidence from other restrictive contexts confirms this connection. In El Salvador, the state’s draconian abortion ban has driven many pregnant women and girls to end their own lives. According to a 2014 report, suicide accounts for 57% of deaths of pregnant females aged 10-19 in El Salvador, though due to stigma surrounding adolescent pregnancy and sexuality, this number may be much higher than reported. Amnesty International, “On the Brink of Death: Violence Against Women and the Abortion Ban in El Salvador” (25 Sept. 2014), https://www.amnesty.org/en/documents/AMR29/003/2014/en/.
[54] See e.g., J. Rovner, “Women Who Tried to Commit Suicide While Pregnant Gets Bail,” NPR (18 May 2022), https://www.npr.org/sections/health-shots/2012/05/18/153026015/bail-granted-for-indiana-woman-charged-in-attempted-feticide (discussing a woman who, under pre-Dobbs laws, was arrested for murder after she attempted suicide while pregnant and her baby died after being born). See also Pregnancy Justice, “When Fetuses Gain Personhood: Understanding the Impact on IVF, Contraception, Medical Treatment, Criminal Law, Child Support, and Beyond” (17 Aug. 2022), https://pregjustdev.wpengine.com/wp-content/uploads/2022/08/Fetal-Personhood-Issue-8.17.22.pdf. See also “Who Do Fetal Homicide Laws Protect? An Analysis for a Post-Roe America,” Pregnancy Justice (9 Jan. 2023), https://www.pregnancyjusticeus.org/wp-content/uploads/2022/08/Feticide-Brief-w-Appendix.pdf.
[55] Bei Bei Shuai v. State of Indiana, No. 49A02–1106–CR–486, Court of Appeals of Indiana (2012).
[56] See R. Baldwin III, “Losing a pregnancy could land you in jail in post-Roe America,” NPR (3 July 2022), https://www.npr.org/2022/07/03/1109015302/abortion-prosecuting-pregnancy-loss (stating that the number of cases where pregnancy or pregnancy loss was used in a criminal investigation or prosecution nearly quadrupled from 2006-2020).
[57] See K. L. Gilbert et al., “Dobbs, another frontline for health equity,” Brookings Institution (30 June 2022), https://www.brookings.edu/blog/how-we-rise/2022/06/30/Dobbs-another-frontline-for-health-equity/ (“Reducing access to abortions does not reduce the number of abortions, rather, it has the effect of reducing access to reproductive health care.”). See also J. Christensen & T. Sneed, “At least 43 abortion clinics shut in month after Supreme Court overturned Roe, research says, with more likely to close,” CNN (28 July 2022), https://www.cnn.com/2022/07/28/health/abortion-clinics-shut-guttmacher/index.html; C. Vestal, “New Research Shows State Restrictions Reduce Contraception Use,” Pew (22 Sept. 2022), https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2022/09/22/new-research-shows-state-restrictions-reduce-contraception-use; M. Ollove, “Critics Fear Abortion Bans Could Jeopardize Health of Pregnant Women,” Pew (22 June 2022), https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2022/06/22/critics-fear-abortion-bans-could-jeopardize-health-of-pregnant-women.
[58]See M. Zahn, “Abortion clinics in embattled states face another challenge: Money,” ABC News (15 Aug. 2022), https://abcnews.go.com/Business/abortion-clinics-embattled-states-face-challenge-money/story?id=87945089 (“Many abortion clinics now must choose between two costly options: stay open but stop providing abortions, or move to an abortion-friendly state, clinic officials and reproductive health organizations told ABC News.”).
[59] Id.
[60] See O. Goldhill, “After Dobbs, U.S. medical students head abroad for abortion training no longer provided by their schools,” STAT (22 Oct. 2022), https://www.statnews.com/2022/10/18/medical-students-heading-abroad-for-abortion-training/ (detailing how medical schools in states with abortion bans are pairing up with programs in other states that allow abortions in an attempt to ensure that future doctors are adequately prepared. Many students interested in reproductive healthcare are considering moving to states where abortions are legal.).
[61] K. Vinekar et al., Projected Implications of Overturning Roe v Wade on Abortion Training in U.S. Obstetrics and Gynecology Residency Programs, 140(2) Obstetrics & Gynecology 146 (2022), p. 147.
[62] J. Hoffman, “OB-GYN Residency Programs Face Tough Choice on Abortion Training,” New York Times (27 Oct 2022) https://www.nytimes.com/2022/10/27/health/abortion-training-residency-programs.html. See also Interview by Physicians for Human Rights with Allison Lenselink (24 Nov. 2022).
[63] “Health coverage if you're pregnant, plan to get pregnant, or recently gave birth,” HealthCare.Gov, https://www.healthcare.gov/what-if-im-pregnant-or-plan-to-get-pregnant/ (last accessed: 10 Jan. 2023).
[64] M. Clark & A. Osorio, Medicaid Pregnancy Coverage Fills a Critical Health Insurance Gap During Pandemic, Data Shows, Georgetown University Health Policy Institute (31 Mar. 2022), https://ccf.georgetown.edu/2022/03/31/medicaid-pregnancy-coverage-fills-a-critical-health-insurance-gap-during-pandemic-data-shows/.
[65] March of Dimes, “Health insurance during pregnancy,” https://www.marchofdimes.org/find-support/topics/planning-baby/health-insurance-during-pregnancy (last accessed: 10 Jan. 2023).
[66] M. Boone & B. J. McMichael, State-Created Fetal Harm, 109 The Georgetown L. Journal 475 (2021), pp. 496-98.
[67] Id.
[68] Id., p. 501.
[69] F. Sellers & F. Nirappil, “Confusion post-Roe spurs delays, denials for some lifesaving pregnancy care,” The Washington Post (16 July 2022), https://www.washingtonpost.com/health/2022/07/16/abortion-miscarriage-ectopic-pregnancy-care/.
[70] L. Paltrow & J. Flavin, Arrests of and Forced Interventions on Pregnant Women in the United States, 1973–2005: Implications for Women's Legal Status and Public Health, Journal of Health Politics, Policy and Law, https://read.dukeupress.edu/jhppl/article/38/2/299/13533/Arrests-of-and-Forced-Interventions-on-Pregnant.
[71] “West Virginia’s only abortion clinic stops performing abortions,” The Associated Press (24 June 2022), https://www.wsaz.com/2022/06/24/west-virginias-only-abortion-clinic-stops-performing-abortions/.
[72] N. Lakhani, “Abortion is still legal in Arizona. But confusion and fear abound,” The Guardian (15 Aug. 2022), https://www.theguardian.com/us-news/2022/aug/15/arizona-abortion-laws-ban-access.
[73] Id.
[74] “Hospitals Fear Abortion Bans Will Worsen Staff Shortages,” Bloomberg Law (updated 9 Aug. 2022), https://news.bloomberglaw.com/health-law-and-business/hospitals-fear-abortion-bans-will-worsen-staff-shortages (“fears of being arrested for prescribing medications that could be unsafe for pregnancy, or for advising chemotherapy that requires ending a pregnancy… ‘The irony is that in states that pass these anti-abortion laws, there will be fewer OB GYN doctors willing to practice there. But there will be more need for them because there will be more pregnancies going to term,’ said Suzanna Sherry, a constitutional law expert at Vanderbilt University Law School.”).
[75] K. Schorsch, “Staffing shortages in Illinois for abortion care,” NPR-WBEZ (12 May 2022), npr.org/local/309/2022/05/12/1098469190/staffing-shortages-in-illinois-for-abortion-care (“Illinois providers are expecting an additional 20,000 to 30,000 patients a year as people travel from other states that could ban or heavily restrict the procedure. That would be a nearly two-thirds increase in abortions across Illinois.” An Illinois doctor cites the healthcare worker shortage as “perhaps the biggest barrier to a full-scale increase that would meet the needs of folks coming from other states.”).
[76] Interview by Foley Hoag LLP with Dr. Elissa Serapio (29 July 2022). See also E. Reyes, “These California Nurse-Midwives Want to Provide Abortions. They’re Struggling to Get Trained,” Los Angeles Times (18 July 2022), latimes.com/california/story/2022-07-18/california-nurse-midwives-want-to-provide-abortions-struggling-to-get-trained.
[77] See S. Aksel et al., Unintended Consequences: Abortion Training in the Years after Roe v Wade, 103Am. J. Public Health 3 (2013) (explaining how provider shortages have created barriers to abortion access); American College of Obstetricians & Gynecologists, Committee Opinion: Abortion Training and Education (Nov. 2014), https://www.acog.org/-/media/project/acog/acogorg/clinical/files/committee-opinion/articles/2014/11/abortion-training-and-education.pdf (Healthcare providers face institutional barriers in getting trained to perform abortions); E. Declercq et al., “The U.S. Maternal Health Divide: The Limited Maternal Health Services and Worse Outcomes of States Proposing New Abortion Restrictions,” The Commonwealth Fund (14 Dec. 2022), https://www.commonwealthfund.org/publications/issue-briefs/2022/dec/us-maternal-health-divide-limited-services-worse-outcomes (maternity care providers may hesitate to work in scenarios where they may face legal challenges).
[78] See generally D. Cohen & K. Connon, Living in the Crosshairs : the Untold Stories of Anti-Abortion Terrorism (2015) (in-depth accounts and data regarding the violence and harassment endured by women's health professionals).
[79] Id.
[80] National Abortion Federation, 2021 Violence & Disruption Statistics (19 May 2022), https://prochoice.org/wp-content/uploads/2021_NAF_VD_Stats_Final.pdf. See also U.S. Dept. of Justice, Recent Cases on Violence Against Reproductive Health Care Providers (updated 18 Oct. 2022), https://www.justice.gov/crt/recent-cases-violence-against-reproductive-health-care-providers.
[81] A January 2020 unclassified report from the FBI outlined an ongoing increase in anti-abortion threats, disruption and violence, stating, “The FBI assess the increase in abortion-related extremist violent threats and criminal activity, including violations of the Freedom of Access to Clinic Entrances (FACE) Act, against targets including reproductive healthcare facilities (RHCFs) likely is driven in part by the recent rise in state legislative activities related to abortion services and access.” (emphasis added); National Abortion Federation, 2020 Violence & Disruption Statistics (2021), p. 2, https://prochoice.org/our-work/provider-security/#dflip-df_13683/3/.
[82] See supra note 87. See also J. Winter, “The Link Between the Capitol Riot and Anti-Abortion Extremism,” The New Yorker (11 Mar. 2021), https://www.newyorker.com/news/daily-comment/the-link-between-the-capitol-riot-and-anti-abortion-extremism; C. Sherman, “Anti-Abortion Activists Were All Over the Capitol Riots,” Vice News (12 Jan. 2021), https://www.vice.com/en/article/4ad73w/anti-abortion-activists-were-all-over-the-capitol-riots.
[83] No patients or staff were present during the attack; a firefighter sustained life threatening injuries. T. Bella, “Arson Suspected at Illinois Planned Parenthood After State Expands Abortion Rights,” Washington Post (19 Jan. 2023), https://www.washingtonpost.com/nation/2023/01/19/abortion-planned-parenthood-arson-illinois/.
[84] See Tex. Health & Safety Code §170A.004, La. Stat. Ann. §14:87.7 (2022), Idaho Code §18-622 (2022), Ala. Code § 26-23H, Ark. Code Ann. § 5-61-304, Ky. Rev. Stat. § 311.772, § 188.017 R.S.Mo., Okla. Stat. tit. 63, § 1-731.4, Miss. Code Ann. § 41-41-45, S.D. Codified Laws § 22-17-5.1, Tenn. Code Ann. § 39-15-201, Wis. Stat. Ann. § 940.04, W. Va. Code § 61-2-8 (currently under an injunction).
[85] The Texas abortion ban classifies any attempt to induce an abortion as a second-degree felony if unsuccessful (punishable by up to 20 years in prison) and as a first degree felony (up to life in prison) “if an unborn child dies as a result of the offense.” Tx. Code § 170A.004(b).
[86] Okla. Stat. tit. 63, § 1-731.4.
[87] For example, Texas’s pre-Roe abortion ban explicitly included accomplice liability (“Whoever furnishes the means for procuring an abortion knowing the purpose intended is guilty as an accomplice”) Tex. Pen. Code art. 1192 (1925), https://www.sll.texas.gov/assets/pdf/historical-statutes/1925/1925-3-penal-code-of-the-state-of-texas.pdf#page=279. Other states, in defining abortion as a felony, have imported generally applicable aiding and abetting provisions. See, e.g., Guidance for Oklahoma law enforcement following Dobbs v. Jackson Women’s Health Org (31 Aug. 2022) (citing Oklahoma definitions of principal and accessory criminal liability, and opining, “Oklahoma law prohibits aiding and abetting the commission of an unlawful abortion, which may include advising a pregnant woman to obtain an unlawful abortion. See 21 O.S. §§ 171-172, 861…”). Meanwhile, Alabama, Arizona, Arkansas, Florida, and Ohio have considered such a provision. See H.B. 4327, 2022 Leg., Reg. Sess. (Okla. 2022); H.B. 23, 2022 Leg., Reg. Sess. (Ala. 2022); H.B. 2483, 55th Leg., 2nd Reg. Sess. (Ariz. 2022); S.B. 13, 93rd Gen. Assemb., 2nd Extraordinary Sess. (Ark. 2021); H.B. 167, 124th Leg., Reg. Sess. (Fla. 2022); H.B. 480, 134th Gen. Assemb., Reg. Sess. (Ohio 2021). See also J. Tolentino, “We’re Not Going Back to the Time Before Roe. We’re Going Somewhere Worse,” The New Yorker (24 June 2022), https://www.newyorker.com/magazine/2022/07/04/we-are-not-going-back-to-the-time-before-roe-we-are-going-somewhere-worse/amp.
[88] R. Klitzman, “Opinion: Roe’s reversal doesn’t just hurt women – it harms us all,” CNN (25 June 2022), https://www.cnn.com/2022/06/25/opinions/medical-ethics-post-roe-world-klitzman/index.html. See also J. Tolentino, “We’re Not Going Back to the Time Before Roe. We’re Going Somewhere Worse,” The New Yorker (24 June 2022), https://www.newyorker.com/magazine/2022/07/04/we-are-not-going-back-to-the-time-before-roe-we-are-going-somewhere-worse/amp. Virtually all of the “trigger laws” punish those conducting and/or aiding an abortion. See also A. Zablocki & M. Sutrina, “The Impact of State Laws Criminalizing Abortion,” Lexis Nexis (27 Sept. 2022), https://www.lexisnexis.com/community/insights/legal/practical-guidance-journal/b/pa/posts/the-impact-of-state-laws-criminalizing-abortion (Noting potential aiding and abetting liability for employers who provide support or time off for employees to obtain abortions; for medical personnel who advise or assist; for individuals who facilitate; or for health plans that cover the procedure); K.E. Queram, “Lyft and Uber Establish Legal Funds to Protect Drivers from Texas Abortion Law,” Route Fifty (7 Sept. 2021), https://www.route-fifty.com/management/2021/09/ride-share-abortion-legal-fund-texas/185154/. T. O’Donnell, “Under Texas ban, private citizens could sue a cab driver who takes a woman to an abortion,” (1 Sept. 2021), https://theweek.com/science/health/1004413/under-texas-ban-private-citizens-could-sue-a-cab-driver-who-takes-a-woman-to; R. Alta Charo, Vigilante Injustice — Deputizing and Weaponizing the Public to Stop Abortions, The New England Journal of Medicine (14 Oct. 2021), https://www.nejm.org/doi/full/10.1056/NEJMp2114886.
[89] A. Zablocki & M. Sutrina, “The Impact of State Laws Criminalizing Abortion,” Lexis Nexis (27 Sept. 2022), https://www.lexisnexis.com/community/insights/legal/practical-guidance-journal/b/pa/posts/the-impact-of-state-laws-criminalizing-abortion; Madiba Denney & Jackie Fielding, “Miscarriage of Justice: The Danger of Laws Criminalizing Pregnancy Outcomes” The Brennan Center (9 Nov. 2021), https://www.brennancenter.org/our-work/analysis-opinion/miscarriage-justice-danger-laws-criminalizing-pregnancy-outcomes.
[90] Texas Heartbeat Act, Senate Bill 8 (SB 8) (20 Mar. 2021) (An Act relating to abortion, including abortions after detection of an “unborn child’s heartbeat”; authorizing a private civil right of action), https://capitol.texas.gov/tlodocs/87R/billtext/pdf/SB00008F.pdf. See also Okla. Stat. tit. 63, §1-745.33-.34, .38 (2022); Idaho Code §§ 18-8804, 18-8807
[91] Tex. Health & Safety Code §§ 170A.001-7 (2022). See id., § I (B)(1).
[92]J. Gerson, “‘No one wants to get sued’: Some abortion providers have stopped working in Texas” The 19th (15 Sept. 2021), https://19thnews.org/2021/09/abortion-providers-texas-stopped-working-under-threat-sued/ (“‘Even if abortion providers win in every single case brought against them [under SB 8], that burden of having to have a lawyer to defend yourself, traveling all over the state to do so — that alone threatens to shut down abortion providers,’ said Marc Hearron, senior counsel at the Center for Reproductive Rights”). In December 2022, a Texas court dismissed a suit from an unaffected, out of state plaintiff against a doctor who had performed an abortion in defiance of the law. The court held that the plaintiff lacked standing to bring the case, but left the door open for plaintiffs with ties to a case to sue providers. See D. Solomon, “Texas’s Abortion ‘Bounty’ Law Just Lost Its First Test. Here’s What That Means,” Texas Monthly (9 Dec. 2022), https://www.texasmonthly.com/news-politics/texas-abortion-bounty-law-just-lost-first-test/.
[93] Interview by Foley Hoag LLP with Dr. Elissa Serapio (25 July 2022). Others involved in abortion care, including lawyers, have the same concerns. I. Mitchell, “Texas Freedom Caucus Warns Law Firm of Criminal Liability for Covering Employees’ Abortion Costs,” The Texan (11 July 2022), available at https://thetexan.news/texas-freedom-caucus-warns-law-firm-of-criminal-liability-for-covering-employees-abortion-costs/ (members of the Texas Freedom Caucus promise to file legislation in the upcoming session to “require the State Bar of Texas to disbar any lawyer that has violated Texas abortion laws.”). See also E. Bowman, “As states ban abortion, the Texas bounty law offers a way to survive legal challenges,” NPR (11 July 2022), https://www.npr.org/2022/07/11/1107741175/texas-abortion-bounty-law. See also M. Kornfield, “A website for ‘whistleblowers’ to expose Texas abortion providers was taken down-again” (6 Sept. 2021), https://www.washingtonpost.com/nation/2021/09/06/texas-abortion-ban-website/.
[94] R. Cohen, “The coming legal battles of post-Roe America,” Vox (27 June 2022), https://www.vox.com/2022/6/27/23183835/roe-wade-abortion-pregnant-criminalize.
[95] C. Kitchener & D. Barrett, “Antiabortion Lawmakers Want to Block Patients from Crossing State Lines,” Washington Post (30 June 2022), https://www.washingtonpost.com/politics/2022/06/29/abortion-state-lines/. See also A. Ollstein & M. Messerly, “Missouri wants to stop out-of-state abortions. Other states could follow,” https://www.politico.com/news/2022/03/19/travel-abortion-law-missouri-00018539 for specific of the Missouri proposal.
[96] M.O. SB603, 101st Gen. Assemb., Reg. Sess. (2021).
[97] See R. Cohen, “The coming legal battles of post-Roe America,” Vox (27 June 2022), https://www.vox.com/2022/6/27/23183835/roe-wade-abortion-pregnant-criminalize. See also S. Ballentine & J. Hanna, “Missouri considers law to make illegal to ‘aid or abet’ out-of-state abortion,” PBS (16 Mar. 2022), https://www.pbs.org/newshour/politics/missouri-considers-law-to-make-illegal-to-aid-or-abet-out-of-state.
[98] T. Gross, “The U.S. faces 'unprecedented uncertainty' regarding abortion law, legal scholar says,” NPR (updated 18 Jan. 2023), https://www.npr.org/sections/health-shots/2023/01/17/1149509246/the-u-s-faces-unprecedented-uncertainty-regarding-abortion-law-legal-scholar-sa; T. Benson, “Interstate Travel Post-Roe Isn’t as Secure as You May Think,” Wired (25 July 2022), https://www.wired.com/story/insterstate-travel-abortion-post-roe/.
[99] Pregnancy-related prosecutions not only existed but were increasing before Dobbs. See Pregnancy Justice, “Arrests and Prosecutions of Pregnant Women, 1973-2020” (18 Sept. 2021), https://www.nationaladvocatesforpregnantwomen.org/wp-content/uploads/2021/09/FINAL_1600cases-Factsheet.docx.pdf. See also M. Goldberg, “When a Miscarriage Is Manslaughter,” The New York Times (18 Oct. 2021), https://www.nytimes.com/2021/10/18/opinion/poolaw-miscarriage.html.
[100] See A. Yurkanin, “Women can be prosecuted for taking abortion pills, says Alabama attorney general,” AL.com (10 Jan. 2023).
[101] Idaho Code §18-606.
[102] Pregnancy Justice, “When Fetuses Gain Personhood: Understanding the Impact on IVF, Contraception, Medical Treatment, Criminal Law, Child Support, and Beyond” (17 Aug. 2022), https://pregjustdev.wpengine.com/wp-content/uploads/2022/08/Fetal-Personhood-Issue-8.17.22.pdf. See also Pregnancy Justice, “Who Do Fetal Homicide Laws Protect? An Analysis for a Post-Roe America,” https://www.nationaladvocatesforpregnantwomen.org/wp-content/uploads/2022/08/Feticide-Brief-w-Appendix.pdf.
[103] International human rights law (IHRL) makes clear that its protections start at birth and that fetal personhood has no basis in IHRL. See Working Group on discrimination against women and girls in law and practice, Women's Autonomy, Equality and Reproductive Health in International Human Rights: Between Recognition, Backlash and Regressive Trends (Oct. 2017), https://www.ohchr.org/sites/default/files/Documents/Issues/Women/WG/WomensAutonomyEqualityReproductiveHealth.pdf (“It was well settled in the 1948 [Universal Declaration of Human Rights] and upheld in the ICCPR that the human rights accorded under IHRL are accorded to those who have been born. ‘All human beings are born free and equal in dignity and rights. They are endowed with reason and conscience and should act towards one another in a spirit of brotherhood.’”). The Working Group cites inter alia the travaux préparatoires of Article 6 of the ICCPR, in which proposed amendments suggesting that the right to life applied before birth were specifically rejected by states. UN GAOR, 12th Session, Agenda Item 33, at 119 (e), (q), UN Doc. A/3764, 1957.
[104] M. Carlisle, “Fetal Personhood Laws Are a New Frontier in the Battle Over Reproductive Rights,” Time (28 June 2022), https://time.com/6191886/fetal-personhood-laws-roe-abortion/. Fetal personhood provisions could also lead to non-abortion-related conduct being criminalized. https://www.usnews.com/news/national-news/articles/2022-05-06/the-push-to-make-fetuses-people-and-abortion-murder/.
[105] O. Gonzalez, “Louisiana abortion bill allowing homicide charges against patients stopped for now,” Axios (13 May 2022), https://www.axios.com/2022/05/13/louisiana-abortion-bill-homicide-patient-roe.
[106] A Tennessee trigger law that will go into effect in August will make performing an abortion a felony that comes with a sentence of up to 15 years imprisonment. A.Sainz & K. Kruesi, “Memphis council resolution addresses abortion prosecutions,” The Associated Press (12 July 2022), https://apnews.com/article/abortion-2022-midterm-elections-us-supreme-court-health-nashville-92c4834b3b0fd10e487c2bc75020c03d. A 2021 study from the National Association of Criminal Defense Lawyers and Pregnancy Justice determined that there are thousands of federal and state crimes already on the books that prosecutors can and have used to charge pregnant persons in a post-Roe world. See National Association of Criminal Defense Lawyers and National Foundation for Criminal Justice, “Abortion in America: How Legislative Overreach Is Turning Reproductive Rights Into Criminal Wrongs” (Aug. 2021), https://www.nacdl.org/getattachment/ce0899a0-3588-42d0-b351-23b9790f3bb8/abortion-in-america-how-legislative-overreach-is-turning-reproductive-rights-into-criminal-wrongs.pdf.
[107] “Alabama Mother Prosecuted for Taking Prescription During Pregnancy,” Equal Justice Initiative (12 July 2021), https://eji.org/news/alabama-mother-prosecuted-for-taking-prescription-during-pregnancy/.
[108] L. Paltrow & L. Sangoi, “The dangerous state laws that are punishing pregnant people,” Think Progress (28 Sept. 2016), https://archive.thinkprogress.org/criminalization-pregnancy-us-43e4741bb514/; Amnesty International, “USA: Criminalizing pregnancy: policing pregnant women who use drugs in the USA” (23 May 2017) https://www.amnesty.org/en/documents/amr51/6203/2017/en/.
[109] “Alabama Mother Prosecuted for Taking Prescription During Pregnancy,” Equal Justice Initiative (12 July 2021), https://eji.org/news/alabama-mother-prosecuted-for-taking-prescription-during-pregnancy/; P. Salhotra, “Does a fetus count in the carpool lane? Texas’ abortion law creates new questions about legal personhood,” The Texas Tribune (13 Sept. 2022), https://www.texastribune.org/2022/09/13/texas-personhood-laws-abortion-law/; M. Carrizosa, “Beyond Abortion: The Fight Over Fetal Personhood Is Here (Video),” Bloomberg Law (12 Jan. 2023), https://news.bloomberglaw.com/us-law-week/beyond-abortion-the-fight-over-fetal-personhood-is-here-video.
[110] See N. Martin, “Take a Valium, Lose Your Kid, Go to Jail,” ProPublica (23 Sept. 2015), https://www.propublica.org/article/when-the-womb-is-a-crime-scene.
[111] See Pregnancy Justice, “Confronting Pregnancy Criminalization: A Practical Guide for Healthcare Providers, Lawyers, Medical Examiners, Child Welfare Workers, and Policymakers,” p. 6 (July 2022), https://www.pregnancyjusticeus.org/wp-content/uploads/2022/06/1.Confronting-PregnancyCriminalization_6.22.23-1.pdf; Pregnancy Justice, “Arrests and Other Deprivations of Liberty of Pregnant Women, 1973-2020,” https://www.pregnancyjusticeus.org/wp-content/uploads/2021/09/FINAL_1600cases-Factsheet.docx.pdf.
[112] See Pregnancy Justice, “Wisconsin’s ‘Unborn Children Protection Act’ (Act 292)” (16 May 2022), https://www.nationaladvocatesforpregnantwomen.org/fact-sheet-wisconsins-unborn-child-protection-act-act.
[113] See Idaho 18-622(5) “Nothing in this section shall be construed to subject a pregnant woman on whom any abortion is performed or attempted to any criminal conviction and penalty.”; S. Harris, “Local woman facing 10 years in prison for allegedly using meth the day she gave birth” (6 June 2021), https://www.idahostatejournal.com/news/local/local-woman-facing-10-years-in-prison-for-allegedly-using-meth-the-day-she-gave/article_e03d4800-cf40-5263-a7d3-085d2d7df2b4.html/; L. Miranda et al., “How States Handle Drug Use During Pregnancy” (30 Sept. 2015), https://projects.propublica.org/graphics/maternity-drug-policies-by-state.
[114] Report of the Working Group on Arbitrary Detention on its visit to the United States of America, ¶ 74 (U.N. Doc. A/HRC/36/37/Add.2) (17 July 2017).
[115] See NWHN Staff, “Consumer Health Info: Medication Abortion and Miscarriage” (updated 15 Aug. 2019), https://nwhn.org/abortion-pills-vs-miscarriage-demystifying-experience/ (“From a medical perspective, there is no physically significant difference between a medication abortion and a spontaneously occurring miscarriage. For example, the medicines used in medication abortion are used to help safely manage an incomplete miscarriage.”).
[116] See M. Dennie & J. Fielding, “Miscarriage of Justice: The Danger of Laws Criminalizing Pregnancy Outcomes,” Brennan Center for Justice (9 Nov. 2021), https://www.brennancenter.org/our-work/analysis-opinion/miscarriage-justice-danger-laws-criminalizing-pregnancy-outcomes. P. Thompson & A. Turcios Cruz, “How an Oklahoma women’s miscarriage put a spotlight on racial disparities in prosecutions,” NBC News (5 Nov. 2021).
[117] “Criminal Justice Fact Sheet,” NAACP, https://naacp.org/resources/criminal-justice-fact-sheet; https://www.prisonpolicy.org/blog/2021/10/08/indigenouspeoplesday/ (“In jails, Native people had more than double the incarceration rate of white people, and in prisons this disparity was even greater.”).
[118] L. Paltrow & J. Flavin, Arrests of and Forced Interventions on Pregnant Women in the United States, 1973–2005: Implications for Women's Legal Status and Public Health, Journal of Health Politics, Policy and Law https://read.dukeupress.edu/jhppl/article/38/2/299/13533/Arrests-of-and-Forced-Interventions-on-Pregnant (noting that the socioeconomic status of economically disadvantaged was indicated by the fact that 71 percent qualified for indigent defense).
[119] See National Association of Criminal Defense Lawyers, Race and the War on Drugs (29 Nov. 2022), https://www.nacdl.org/Content/Race-and-the-War-on-Drugs.
[120] Report by the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health: Racism and the right to health (U.N. Doc. A/77/197) (20 July 2022).
[121] See American College of Obstetricians and Gynecologists, Opposition to Criminalization of Individuals During Pregnancy and the Postpartum Period-Statement of Policy (Dec. 2020), https://www.acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2020/opposition-criminalization-of-individuals-pregnancy-and-postpartum-period.
[122] A recent study by If/When/How found “at least 61 instances where people were investigated or prosecuted for allegedly self-managing an abortion or helping others self-manage. Among the cases involving adults, 26% were reported by acquaintances (including family, friends, and neighbors) and 45% were reported by care professionals (including doctors, nurses, and social workers) after seeking care...Whether criminalization has occurred out of malice or simply due to ignorance of reporting requirements, clinicians, social workers, and other clinical support providers have caused substantial harm to patients by calling law enforcement after the loss of pregnancy because they suspect the miscarriage was intentionally induced.” J. Perritt, “Don't Report Your Abortion Patients to Law Enforcement—Self-managed abortion does not legally need to be reported,” Medpage Today (5 Nov. 2022), https://www.medpagetoday.com/opinion/second-opinions/101581; (citing L. Huss et al., Self-Care, Criminalized: August 2022 Preliminary Findings, If How When: Lawyering for Reproductive Justice 2-3 (2022)). See also E. Bazelon, “Purvi Patel Could Be Just the Beginning,” The New York Times (1 Apr. 2015), https://www.nytimes.com/2015/04/01/magazine/purvi-patel-could-be-just-the-beginning.html.
[123] S. Artiga et al., “Racial Disparities in Maternal and Infant Health: An Overview,” Kaiser Family Foundation (10 Nov. 2020), https://www.kff.org/report-section/racial-disparities-in-maternal-and-infant-health-an-overview-issue-brief/.
[124] E. Yuko, “Women of Color Will Face More Criminalized Pregnancies in Post-‘Roe’ America,” Rolling Stone (7 July 2022), https://www.rollingstone.com/culture/culture-features/roe-wade-abortion-criminalized-pregnancy-bipoc-1377430/.
[125] Working Group on discrimination against women and girls in law and practice, Women’s Autonomy, Equality and Reproductive Health in International Human Rights: Between Recognition, Backlash and Regressive Trends (Oct. 2017), https://www.ohchr.org/sites/default/files/Documents/Issues/Women/WG/WomensAutonomyEqualityReproductiveHealth.pdf.
[126] See, e.g., C. Zakrzewski et al., “Texts, web searches about abortion have been used to prosecute women,” The Washington Post (3 July 2022), https://www.washingtonpost.com/technology/2022/07/03/abortion-data-privacy-prosecution/. See also R. Williams, “How might law enforcement use digital tracking to enforce Georgia’s strict anti-abortion law?” GPB (30 Aug. 2022), https://www.gpb.org/news/2022/08/30/how-might-law-enforcement-use-digital-tracking-enforce-georgias-strict-anti.
[127] See K. Cheung, “Abortion in the Surveillance State,” Jezebel (22 Nov. 2021), https://jezebel.com/abortion-in-the-surveillance-state-1848076906. See also J. Schuppe, “Police sweep Google searches to find suspects. The tactic is facing its first legal challenge,” NBC News (30 June 2022), https://www.nbcnews.com/news/us-news/police-google-reverse-keyword-searches-rcna35749.
[128] P. Hurtado et al., “In a Post-Roe World, More Miscarriage and Stillbirth Prosecutions Await Women,” Bloomberg (5 July 2022), https://www.bloomberg.com/news/articles/2022-07-05/miscarriage-stillbirth-prosecutions-await-women-post-roe. See also L. Rankin, “How an online search for abortion pills landed this woman in jail,” Fast Company (26 Feb. 2020), https://www.fastcompany.com/90468030/how-an-online-search-for-abortion-pills-landed-this-woman-in-jail.
[129] Federal Trade Commission, “Data Brokers: A Call for Transparency and Accountability,” p. i (May 2014), https://www.ftc.gov/system/files/documents/reports/data-brokers-call-transparency-accountability-report-federal-trade-commission-may-2014/140527databrokerreport.pdf.
[130] Federal courts have not ruled directly on whether the particularized probable cause standard applicable to warrant requests is required for police to conduct keyword search queries or “geofenced” (i.e. location-bound) searches of data held by third parties, including Google. At the moment, law enforcement is relying on vague and less-protective statutory standards, such as the Stored Communication Act’s “reasonable grounds [to believe that records are] relevant and material to an ongoing investigation” standard. Congressional Research Service, “Abortion, Data Privacy, and Law Enforcement Access: A Legal Overview” (updated 8 July 2022), https://crsreports.congress.gov/product/pdf/LSB/LSB10786.
[131] J. Cox, “Data Broker Is Selling Location Data of People Who Visit Abortion Clinics,” Vice (3 May 2022), https://www.vice.com/en/article/m7vzjb/location-data-abortion-clinics-safegraph-planned-parenthood (reporting on the sale of data “showing where groups of people visiting [clinics the provide abortions] came from, how long they stayed there, and where they then went afterwards.”). See also B. Cyphers, “Inside Fog Data Science, the Secretive Company Selling Mass Surveillance to Local Police,” EFF (31 Aug. 2022), https://www.eff.org/deeplinks/2022/08/inside-fog-data-science-secretive-company-selling-mass-surveillance-local-police (describing how private data brokers sell searchable access to “‘billions’ of data points about ‘over 250 million’ devices” to local law enforcement agencies, generally without any court oversight).
[132] B. Cyphers, “How Law Enforcement Around the Country Buys Cell Phone Location Data Wholesale,” EFF (31 Aug. 2022), https://www.eff.org/deeplinks/2022/08/how-law-enforcement-around-country-buys-cell-phone-location-data-wholesale Some data broker services are designed and marketed specifically for law enforcement agencies, who purchase subscriptions to the services – rather than seeking a warrant – in order to access advanced search features. The Electronic Frontier Foundation documented a lack of agency-level policies governing the use of these services, and found that most agencies did not seek either warrants or subpoenas to access the data. See also F. Patel & A. Shahzad, “With Roe v. Wade at Risk, Digital Surveillance Threatens Reproductive Freedom,” Just Security (17 May 2022), https://www.justsecurity.org/81547/with-roe-v-wade-at-risk-digital-surveillance-threatens-reproductive-freedom/.
[133] S. Quenby et al., “Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss,” The Lancet (Vol. 397, 2021), p. 1658; D. Walker, “With Roe overturned, Indigenous communities say it was always impossible for them to access abortion services,” Insider (24 June 2002), https://www.insider.com/roe-overturned-harder-for-indigenous-communities-to-access-abortion-2022-5.
[134] National Women’s Health Center, “Consumer Health Info: Medication Abortion and Miscarriage” (updated 15 Aug. 2019), https://nwhn.org/abortion-pills-vs-miscarriage-demystifying-experience/ (“From a medical perspective, there is no physically significant difference between a medication abortion and a spontaneously occurring miscarriage. For example, the medicines used in medication abortion are used to help safely manage an incomplete miscarriage.”).
[135] C. Conti-Cook, Surveilling the Digital Abortion Diary, 50 (1) University of Baltimore Law Review 1 (2020), pp. 29-38.
[136] See M. Gilman, The Class Differential in Privacy Law, 77 Brook. L. Rev. 1389, 1392 (2012), https://brooklynworks.brooklaw.edu/blr/vol77/iss4/2.
[137] See E. Joh, Dobbs Online: Digital Rights as Abortion Rights (5 Sept. 2022) (feminist cyberlaw, A. Levendowski & M. Jones (eds.), forthcoming 2023), https://ssrn.com/abstract=4210754) (noting that low-income women are less able to afford more privacy-protective phones, apps, or other services).
[138] See K. Cheung, “Abortion in the Surveillance State,” Jezebel (22 Nov. 2021), https://jezebel.com/abortion-in-the-surveillance-state-1848076906; S. Coutts, “Anti-Choice Groups Use Smartphone Surveillance to Target ‘Abortion-Minded Women’ During Clinic Visits,” Rewire News Group (25 May 2016), https://rewirenewsgroup.com/2016/05/25/anti-choice-groups-deploy-smartphone-surveillance-target-abortion-minded-women-clinic-visits/.
[139] A. Abrams & V. Bergengruen, “Anti-Abortion Pregnancy Centers Are Collecting Troves of Data That Could Be Weaponized Against Women,” Time (22 June 2022), https://time.com/6189528/anti-abortion-pregnancy-centers-collect-data-investigation/.
[140] J. Cox, “Data Broker Is Selling Location Data of People Who Visit Abortion Clinics,” Vice (3 May 2022), https://www.vice.com/en/article/m7vzjb/location-data-abortion-clinics-safegraph-planned-parenthood; E. Joh, Dobbs Online: Digital Rights as Abortion Rights (5 Sept. 2022) (A. Levendowski & M. Jones (eds.), feminist cyberlaw, forthcoming 2023), https://ssrn.com/abstract=4210754). See also A. Vesoulis, “How a Digital Abortion Footprint Could Lead to Criminal Charges—And What Congress Can Do About It,” Time (10 May 2022), available at https://time.com/6175194/digital-data-abortion-congress/; E. Bowman, “As states ban abortion, the Texas bounty law offers a way to survive legal challenges,” NPR (11 July 2022), https://www.npr.org/2022/07/11/1107741175/texas-abortion-bounty law#:~:text=The%20law%20makes%20no%20exceptions,%2410%2C000%20in%20damages%20from%20defendants.
[141] See J. Cox, “Data Broker Is Selling Location Data of People Who Visit Abortion Clinics,” Vice (3 May 2022), https://www.vice.com/en/article/m7vzjb/location-data-abortion-clinics-safegraph-planned-parenthood. Following the initial story, this particular data broker announced it would cease selling data specifically tracking those who visited abortion providers, and subsequently eliminated retail access to its data altogether; however, nothing prevents other brokers from offering identical products. J. Cox, “SafeGraph to Close Digital Shop That Sold Abortion Clinic Location Data,” Vice (30 Sept. 2022), https://www.vice.com/en/article/g5vw3b/safegraph-to-close-shop-abortion-clinic-location-data.
[142] N. Poli & V. Bergengruen, “Lawmakers Scramble to Reform Digital Privacy After Roe Reversal,” Time (1 July 2022), https://time.com/6193224/abortion-privacy-data-reform/.
[143] Complaint, Generation to Generation Inc. v. State of Florida, No. 2022-CA-000980 (Leon Cty. Fla., Circ. Ct., 10 June 2022). See also E. Fawcett, “Synagogue Sues Florida, Saying Abortion Restrictions Violate Religious Freedoms,” The New York Times (16 June 2022), https://www.nytimes.com/2022/06/16/us/florida-abortion-law-judaism.html.
[144] The providers in Florida who have resorted to the courts to assert their right to freedom of religion or belief are part of a long tradition of healthcare workers providing reproductive healthcare, at least in part, due to their faith. See A Religious Right to Abortion: Legal History and Analysis, Columbia Law School (Aug. 2022), https://lawrightsreligion.law.columbia.edu/sites/default/files/content/LRRP%20Religious%20Liberty%20%26%20Abortion%20Rights%20memo.pdf.
[145] M. Boorstein, “Clergy sue to halt Florida abortion law, citing religious freedom,” The Washington Post (1 Sept. 2022), https://www.washingtonpost.com/religion/2022/09/01/florida-pastor-rabbi-abortion-lawsuit/.
[146] Id.
[147] UN General Assembly, International Covenant on Civil and Political Rights (16 Dec. 1966), United Nations, Treaty Series (Vol. 999) (“ICCPR”), https://www.refworld.org/docid/3ae6b3aa0.html [accessed 28 January 2023], Art.18 (3).
[148] See A. Branigin & S. Chery, “Women of color will be most impacted by the end of Roe, experts say,” The Washington Post (24 June 2022), https://www.washingtonpost.com/nation/2022/06/24/women-of-color-end-of-roe/. See also L. Powell, “Human Rights Campaign Fact Sheet: Lesbian, Bisexual, Queer Women Who Have Been Pregnant Are More Likely to Need Abortion Services; Demonstrates Impact Roe Reversal Would Have on LGBTQ+ People,” Human Rights Campaign (2 June 2022), available at https://www.hrc.org/press-releases/human-rights-campaign-fact-sheet-lesbian-bisexual-queer-women-who-have-been-pregnant-are-more-likely-to-need-abortion-services-demonstrates-impact-roe-reversal-would-have-on-lgbtq-people. See also American Association of People with Disabilities, “AAPD Statement on Leaked Supreme Court Draft Decision and Threat to Roe v. Wade” (10 May 2022), https://www.aapd.com/press-releases/aapd-statement-scotus-threat-to-roe/.
[149] See, e.g., E.E. Petersen et al., “Vital Signs: Pregnancy-Related Deaths, United States, 2011–2015, and Strategies for Prevention, 13 States, 2013–2017,” MMWR Morb Mortal Wkly Rep (2019), 68:423–429 (between 2011 and 2015 Indigenous women had the second highest rate of pregnancy-related deaths); M. Long et al., “Women’s Health Care Utilization and Costs: Findings from the 2020 KFF Women’s Health Survey” (21 Apr. 2021), https://www.kff.org/womens-health-policy/issue-brief/womens-health-care-utilization-and-costs-findings-from-the-2020-kff-womens-health-survey (low-income women, Black women, and Hispanic women); G. Borchelt, “The Impact Poverty Has on Women’s Health,” https://www.americanbar.org/groups/crsj/publications/human_rights_magazine_home/the-state-of-healthcare-in-the-united-states/poverty-on-womens-health (low-income women); M. Buckles “Improving Health Outcomes for Black Women and Girls With Disabilities” (15 Feb. 2022), https://www.americanprogress.org/article/improving-health-outcomes-for-black-women-and-girls-with-disabilities (Black women and women with disabilities); L. Johnson, “The Disparate Impact of Texas’ Abortion Ban on Low-Income and Rural Women,” Georgetown Law Journal on Poverty Law and Policy (24 Feb. 2022), https://www.law.georgetown.edu/poverty-journal/blog/the-disparate-impact-of-texas-abortion-ban-on-low-income-and-rural-women (rural and low-income women).
[150] See K.L. Gilbert et al., “Dobbs, another frontline for health equity,” Brookings Institution (30 June 2022), https://www.brookings.edu/blog/how-we-rise/2022/06/30/Dobbs-another-frontline-for-health-equity/. See also D. Walker, “With Roe overturned, Indigenous communities say it was always impossible for them to access abortion services” (24 June 2022), https://www.insider.com/roe-overturned-harder-for-indigenous-communities-to-access-abortion-2022-5; L. Kcomt et al., “Healthcare avoidance due to anticipated discrimination among transgender people: A call to create trans-affirmative environments” (28 May 2020), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7276492/pdf/main.pdf; B. Karami Matin et al., “Barriers in access to healthcare for women with disabilities: a systematic review in qualitative studies” (30 Jan. 2021), https://bmcwomenshealth.biomedcentral.com/track/pdf/10.1186/s12905-021-01189-5.pdf; U. Ranji et al., “Beyond the Numbers: Access to Reproductive Health Care for Low-Income Women in Five Communities” (14 Nov. 2019), https://www.kff.org/report-section/beyond-the-numbers-access-to-reproductive-health-care-for-low-income-women-in-five-communities-executive-summary.; L. Fuentes, “Inequity in US Abortion Rights and Access: The End of Roe is Deepening Existing Divides,” Guttmacher Institute (Jan. 2023), https://www.guttmacher.org/2023/01/inequity-us-abortion-rights-and-access-end-roe-deepening-existing-divides (“Drivers of inequity such as income and health insurance disparities and health provider bias…are not simply the result of individual acts of discrimination but rather the result of how institutions and public infrastructures function.”).
[151] Brief for Autistic Self Advocacy Network and the Disability Rights Education and Defense Fund as Amicus Curiae (Dobbs v. Jackson Women's Health Org., 142 S. Ct. 2228) (20 Sept. 2021), p. 7, https://www.supremecourt.gov/DocketPDF/19/19-1392/192964/20210920135335415_19-1392%20Amicus%20Brief%20of%20The%20Autistic%20Self%20Advocacy%20Network%20et%20al..pdf (“around 60,000 Americans were forcibly sterilized in state-sanctioned programs to prevent those adjudged to have psychiatric disabilities from reproducing”). See also P. Lombardo, Three Generations, No Imbeciles: New Light on Buck v. Bell, 60 N.Y.U. L. Rev. 30, 31 (1985); A. Stern, “Forced sterilization policies in the US targeted minorities and those with disabilities – and lasted into the 21st century,” IHPI News (23 Sept. 2020), https://ihpi.umich.edu/news/forced-sterilization-policies-us-targeted-minorities-and-those-disabilities-and-lasted-21st (“Anyone who did not fit [the] mold of racial perfection, which included most immigrants, Blacks, Indigenous people, poor whites and people with disabilities, became targets of eugenics programs.”); National Women’s Law Center, Forced Sterilization of Disabled People in the United States (24 Jan. 2022), https://nwlc.org/wp-content/uploads/2022/01/%C6%92.NWLC_SterilizationReport_2021.pdf; (Appendix) https://nwlc.org/wp-content/uploads/2022/01/%C6%92.NWLC_SterilizationReport_2022_Appendix.pdf.
[152] Brief for Autistic Self Advocacy Network and the Disability Rights Education and Defense Fund as Amicus Curiae (Dobbs v. Jackson Women's Health Org., 142 S. Ct. 2228) (20 Sept. 2021), p. 7, https://www.supremecourt.gov/DocketPDF/19/19-1392/192964/20210920135335415_19-1392%20Amicus%20Brief%20of%20The%20Autistic%20Self%20Advocacy%20Network%20et%20al..pdf.
[153] L. Bowen, “Dobbs Is a Disaster for Disability Justice,” Society for Cultural Anthropology (3 Oct. 2022), https://culanth.org/fieldsights/Dobbs-is-a-disaster-for-disability-justice. See also R. Hoban, “In debate over Down syndrome/abortion bill, disability groups struggle with how to respond,” North Carolina Health News (8 June 2021), https://www.northcarolinahealthnews.org/2021/06/08/disability-groups-struggle-to-respond-to-latest-abortion-bill/.
[154] M. Smith, “Native Americans: A Crisis in Health Equity,” American Bar Association Human Rights Magazine (Vol. 43, No. 3) (1 Aug. 2018), https://www.americanbar.org/groups/crsj/publications/human_rights_magazine_home/the-state-of-healthcare-in-the-united-states/native-american-crisis-in-health-equity/. The United Nations’ Department for Economic and Social Affairs has also produced reports on indigenous peoples’ access to health services around the world, finding these groups face heightened challenges. See “State of the World’s Indigenous Peoples: Indigenous Peoples’ Access to Health Services,” United Nations Department of Economic and Social Affairs (March 2018), https://www.un.org/development/desa/indigenouspeoples/wp-content/uploads/sites/19/2018/03/The-State-of-The-Worlds-Indigenous-Peoples-WEB.pdf.
[155] E. Hofstaedter, “Abortion Was Already Inaccessible on Reservation Land. Dobbs Made Things Worse,” Mother Jones (12 Aug. 2022), https://www.motherjones.com/politics/2022/08/abortion-Dobbs-tribal-land/.
[156] See D. Williams et al., Understanding and Addressing Racial Disparities in Health Care, 21(4) Health Care Financing Review 75 (2000). See also Key Facts on Health and Health Care by Race and Ethnicity, Kaiser Family Foundation, (26 Jan. 2022), https://www.kff.org/racial-equity-and-health-policy/report/key-facts-on-health-and-health-care-by-race-and-ethnicity/; “Closing the Equity Gap in Health Care for Black Americans,” The Commonwealth Fund (15 July 2016), https://www.commonwealthfund.org/blog/2016/closing-equity-gap-health-care-black-americans. Black women may also be particularly impacted by abortion bans because they have historically been overrepresented among people seeking abortions. See “Reported Legal Abortions by Race of Women Who Obtained Abortion by the State of Occurrence,” Kaiser Family Foundation (2020), https://www.kff.org/racial-equity-and-health-policy/report/key-facts-on-health-and-health-care-by-race-and-ethnicity/
[157] See, e.g., A. Spencer, “Black Rural Residents Lack Healthcare Due to Racism and Poverty,” The Sacramento Observer (22 Aug. 2022), https://sacobserver.com/2022/08/black-rural-residents-lack-healthcare-due-to-racism-and-poverty/.
[158] See “Submission to the United Nations Committee on the Elimination of Racial Discrimination,” Amnesty International, The Global Justice Center, The Southern Rural Black Women’s Initiative for Economic and Social Justice, and Human Rights Watch (Aug. 2022), https://www.hrw.org/sites/default/files/media_2022/07/SBRWI_HRW_GJC_AI_CERDShadowReport.pdf. See A Post-Roe America: The Legal Consequences of the Dobbs Decision: Hearing before the Senate Committee on the Judiciary, 117th Cong. section IV (2022) (statement of Khiara M. Bridges Professor of Law, UC Berkeley School of Law), https://www.judiciary.senate.gov/imo/media/doc/Testimony%20-%20Bridges%20-%202022-07-121.pdf.
[159] See generally A. Bissonnette, “Caged Women”: Migration, Mobility and Access to Health Services in Texas and Arizona, 37 J. Borderlands Studies 1 (9 Apr. 2020), tandfonline.com/doi/abs/10.1080/08865655.2020.1748515?journalCode=rjbs20.
[160] Barriers to sexual and reproductive health services faced by immigrant women of reproductive age in the United States, Ibis Reproductive Health (Jan. 2023), https://www.ibisreproductivehealth.org/sites/default/files/files/publications/Access%20to%20SRH%20services_immigrants%20brief%20FINAL.pdf. Many noncitizen US residents are ineligible for Medicaid and the Children’s Health Insurance Program (CHIP) for their first five years in the country. Health coverage for lawfully present immigrants: Immigrants and Medicaid & CHIP, HealthCare.Gov (17 Jan. 2023), https://www.healthcare.gov/immigrants/lawfully-present-immigrants/.
[161] S. Ahmed, “Abortion worries heightened for unauthorized immigrants in the U.S.,” Reuters (5 July 2022), https://www.reuters.com/world/us/abortion-worries-heightened-unauthorized-immigrants-us-2022-07-05/.
[162] Interview by Foley Hoag LLP with Dr. Elissa Serapio (25 July 2022).
[163] Human Rights Watch, “The Only People It Really Affects Are the People It Hurts” (11 Mar. 2021), https://www.hrw.org/report/2021/03/11/only-people-it-really-affects-are-people-it-hurts/human-rights-consequences.
[164] “Barriers to sexual and reproductive health services faced by immigrant women of reproductive age in the United States,” Ibis Reproductive Health (Jan. 2023), https://www.ibisreproductivehealth.org/sites/default/files/files/publications/Access%20to%20SRH%20services_immigrants%20brief%20FINAL.pdf.
[165] See K.L. Gilbert et al., “Dobbs, another frontline for health equity,” Brookings Institution (30 June 2022), https://www.brookings.edu/blog/how-we-rise/2022/06/30/Dobbs-another-frontline-for-health-equity/; M. Kirstein et al., “100 Days Post-Roe: At Least 66 Clinics Across 15 US States Have Stopped Offering Abortion Care,” Guttmacher Institute (6 Oct. 2022), https://www.guttmacher.org/2022/10/100-days-post-roe-least-66-clinics-across-15-us-states-have-stopped-offering-abortion-care (Noting that abortion bans lead to clinic closures and “[w]hen clinics close down or stop offering abortion care, it represents a lost source of health care for their community.”).
[166] See K. L. Gilbert et al., “Dobbs, another frontline for health equity,” Brookings Institution (30 June 2022), https://www.brookings.edu/blog/how-we-rise/2022/06/30/Dobbs-another-frontline-for-health-equity/ (“Of the 13 states that have an immediate trigger law, 9 of them rank number 30 or lower in overall state health using data from America’s Health Rankings. More than 10 of these states rank in the bottom half for public health and healthcare quality.”).
[167] See National Institute of Justice, “Violence Against American Indian and Alaska Native Women and Men: 2010 Findings From the National Intimate Partner and Sexual Violence Survey,” (May 2016), pp. 2, 14, available at https://www.ojp.gov/pdffiles1/nij/249736.pdf (Indigenous women); S.E. Tan & K. Kuschminder, “Migrant experiences of sexual and gender based violence: a critical interpretative synthesis,” Global Health (2022), pp. 18, 68 (migrant women); “Violence Against Women in the United States: Statistics,” available at https://now.org/resource/violence-against-women-in-the-united-states-statistic (low-income women); J. Barlow “Black women, the forgotten survivors of sexual assault,” https://www.apa.org/pi/about/newsletter/2020/02/black-women-sexual-assault (Black women); R. Dowd “Transgender people over four times more likely than cisgender people to be victims of violent crime,” UCLA School of Law Williams Institute (23 Mar. 2021), https://williamsinstitute.law.ucla.edu/press/ncvs-trans-press-release (transgender men); “Violence and Abuse in Rural America” (last reviewed 26 Mar. 2021), https://www.ruralhealthinfo.org/topics/violence-and-abuse (women in rural communities); CDC, “Sexual Violence and Intimate Partner Violence Among People with Disabilities” (last reviewed 1 June 2020), https://www.cdc.gov/violenceprevention/sexualviolence/svandipv.html (women with disabilities).
[168] Most states with abortion bans in effect do not have any exception for pregnancies that result from rape or incest. F. Cineas, “Rape and incest abortion exceptions don’t really exist,” Vox (22 July 2022), https://www.vox.com/23271352/rape-and-incest-abortion-exception. See, e.g., Alabama Human Life Protection Act (H.B. 314, § 7); Wisconsin § 940.04(5); Wyoming § 35-6-102.(b); Texas Health & Safety Code Title 2, Subtit. H, Ch. 170A; Tennessee Code Ann. § 39-15-213.(c)(1)-(3); South Dakota, § 22-17-5.1; Miss. Code Ann. § 41-41-45.(2) (contemplating rape only); Louisiana § 40:1061.F-G; Kentucky § 311.772.(4)(a)-(b); Arkansas A.C.A. § 5-61-304(a); Arizona A.R.S. § 13-3603.02.A; Oklahoma S.B. 612 Section A.B.3.a; Missouri (§ 188.017 R.S.Mo.).
[169] Most states with a rape exception to their abortion ban require the victim to report the rape to the police in order to obtain an abortion. F. Cineas, “Rape and incest abortion exceptions don’t really exist,” Vox (22 July 2022), https://www.vox.com/23271352/rape-and-incest-abortion-exception.
[170] RAINN, The Criminal Justice System: Statistics, https://www.rainn.org/statistics/criminal-justice-system.
[171] D. Thompson, “When Abortion Means Traveling, More Women Forgo Procedure: Study”, US News (16 May 2022), https://www.usnews.com/news/health-news/articles/2022-05-16/when-abortion-means-traveling-more-women-forgo-procedure-study.
[172] See N. Hassanein, “People of color, the poor and other marginalized people to bear the brunt if Roe v. Wade is overturned,” USA Today (3 May 2022), https://www.usatoday.com/story/news/health/2022/05/03/people-color-most-impacted-if-roe-v-wade-overturned/9626866002/. See also A. Schrager, “No Abortion Means Poor States Will Get Poorer,” The Washington Post (4 May 2022), https://www.washingtonpost.com/business/no-abortion-means-poor-states-will-get-poorer/2022/05/04/276bcde6-cb9a-11ec-b7ee-74f09d827ca6_story.html.
[173] D. Thompson, “When Abortion Means Traveling, More Women Forgo Procedure: Study,” US News (16 May 2022), https://www.usnews.com/news/health-news/articles/2022-05-16/when-abortion-means-traveling-more-women-forgo-procedure-study.
[174] B. Rader MPH et al., Estimated Travel Time and Spatial Access to Abortion Facilities in the US Before and After the Dobbs v Jackson Women’s Health Decision, JAMA 2022;328(20):2041–2047, https://jamanetwork.com/journals/jama/article-abstract/2798215.
[175] See J. Bearak et al., “Disparities and change over time in distance women would need to travel to have an abortion in the USA: a spatial analysis,” Lancet Public Health (Nov. 2017), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5943037/. See also R. Bleiweis et al., “The Basic Facts About Women in Poverty” (3 Aug. 2020), CAP, https://www.americanprogress.org/article/basic-facts-women-poverty; Status of Women in the States, “Spotlight on Immigrant Women: The Employment and Earning of Immigrant Women,” https://statusofwomendata.org/immigrant-women; M.V. Badgett et al., “ LGBT Poverty in the United States,” UCLA School of Law Williams Institute (Oct. 2019), https://williamsinstitute.law.ucla.edu/publications/lgbt-poverty-us; Committee Opinion, “Health Disparities in Rural Women,” The American College of Obstetricians and Gynecologists (Feb. 2014, reaffirmed in 2021), https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2014/02/health-disparities-in-rural-women (rural women).
[176] D. Foster, The Turnaway Study: The Cost of Denying Women Access to Abortion (2020).
[177] D. Foster, New abortion bans will increase existing health and economic disparities, 112 Am. J. Pub. Health 1276 (June 2022), https://ajph.aphapublications.org/doi/10.2105/AJPH.2022.306993.
[178] See United Nations, The State Parties to the International Covenant on Civil and Political Rights (ICCPR), available at https://treaties.un.org/Pages/ViewDetails.aspx?chapter=4&clang=_en&mtdsg_no=IV-4&src=IND (US ratification, 8 June 1992).
[179] See United Nations, The State Parties to the International Convention on the Elimination of All Forms of Racial Discrimination (ICERD), https://treaties.un.org/Pages/ViewDetails.aspx?src=IND&mtdsg_no=IV-2&chapter=4&clang=_en (US ratification, 21 Oct. 1994).
[180] See United Nations, The State Parties to the Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment (CAT), https://www.ohchr.org/sites/default/files/cat.pdf (US ratification, 21 Oct. 1994).
[181] See United Nations, The State Parties to the International Covenant on Economic, Social and Cultural Rights (ICESCR), https://treaties.un.org/Pages/ViewDetails.aspx?src=IND&mtdsg_no=IV-3&chapter=4 (US ratification, 5 Oct. 1977).
[182] See United Nations, The State Parties to the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW), https://treaties.un.org/pages/ViewDetails.aspx?src=IND&mtdsg_no=IV-8&chapter=4&clang=_en (US ratification, 17 July 1980).
[183] See United Nations, The State Parties to the Convention on the Rights of the Child (CRC), https://treaties.un.org/pages/ViewDetails.aspx?src=IND&mtdsg_no=IV-11&chapter=4&clang=_en (US ratification, 16 Feb. 1995).
[184] See United Nations, The State Parties to the Convention on the Rights of Persons with Disabilities (CRPD), https://treaties.un.org/pages/ViewDetails.aspx?chapter=4&clang=_en&mtdsg_no=IV-15&src=IND (US ratification, 30 July 2009).
[185] See United Nations, Vienna Convention on the Law of Treaties (23 May 1969), United Nations, Treaty Series (Vol. 1155) (VCLT), Art. 18.
[186] See Brief of the United Nations Mandate Holders as Amici Curiae, Dobbs v. JWHO., 142 S. Ct. 2228, p. 9 (20 Sept. 2021), https://www.supremecourt.gov/DocketPDF/19/19-1392/193045/20210920163400578_19-1392%20bsac%20United%20Nations%20Mandate%20Holders.pdf.
[187] As recently summarized by the Working Group on discrimination against women and girls: “sexual and reproductive health rights are clearly established under international law. They are an integral part of a number of civil and political rights that underpin the physical and mental integrity of individuals and their autonomy, such as the rights to life, liberty and security of person, freedom from torture and other cruel, inhuman or degrading treatment, privacy and respect for family life, as well as economic, social and cultural rights, such as the rights to health, education and work and the right to enjoy the benefits of scientific progress, and the cross-cutting rights of non-discrimination and equality.” Working Group on discrimination against women and girls, Women’s and girls’ sexual and reproductive health rights in crisis (U.N. Doc. A/HRC/47/38) (28 Apr. 2021), ¶ 18.
[188] See ICCPR, Art. 6.
[189] See ICERD, Art. 5(e)(iv). See also ICESCR Art. 12; CEDAW Arts. 11(1)(f), 12, 14(2)(b); CRPD Art. 25; CRC Art. 24. See also CESCR, General Comment No. 22 (2016) on the right to sexual and reproductive health (U.N. Doc. E/C.12/GC/22) (2 May 2016), ¶¶ 10-11, 13-14, 45, 49; CRC Committee, General comment No. 15 (2013) on the right of the child to the enjoyment of the highest attainable standard of health (U.N. Doc. CRC/C/GC/15) (17 Apr. 2013), ¶ 56; Report of the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health, Violence and its impact on the right to health (U.N. Doc. A/HRC/50/28) (14 Apr. 2022), ¶ 20 (describing how “States violate the right to health when they fail to take effective steps to prevent third parties from undermining the enjoyment of the right to sexual and reproductive health”).
[190] HRC, General Comment No. 36, Art. 6 (Right to Life) (U.N. Doc. CCPR/C/GC/36) (3 Sept. 2019), ¶ 8.
[191] Id.
[192] See CESCR, General Comment 22 (2016) on the right to sexual and reproductive health (U.N. Doc. E/C.12/GC/22) (2 May 2016), ¶ 5 (“The freedoms [protected under the right to health] include the right to make free and responsible decisions and choices, free of violence, coercion and discrimination, regarding matters concerning one’s body and sexual and reproductive health[, and entitle all people to] full enjoyment of the right to sexual and reproductive health[.]”); CESCR, General Comment No. 14: The Right to the Highest Attainable Standard of Health (Art. 12) (U.N. Doc. E/C.12/2000/4) (11 Aug. 2000), ¶ 8 (“The freedoms [protected under the right to health] include the right to control one’s health and body, including sexual and reproductive freedom, and the right to be free from interference[.]”); CRPD Committee and CEDAW Committee, Guaranteeing sexual and reproductive health and rights for all women, in particular women with disabilities (29 Aug. 2018), https://www.ohchr.org/en/treaty-bodies/crpd/statements-declarations-and-observations (“Access to safe and legal abortion, as well as related services and information are essential aspects of women’s reproductive health and a prerequisite for safeguarding their human rights to life, health, equality before the law and equal protection of the law, non-discrimination, information, privacy, bodily integrity and freedom from torture and ill treatment.”); CEDAW Committee, L.C. v. Peru (U.N. Doc. CEDAW/C/50/D/222009) (2011), ¶ 8.15, https://www2.ohchr.org/english/law/docs/cedaw-c-50-d-22-2009_en.pdf (“[T]he Committee considers that, owing to her condition as a pregnant woman, L.C. did not have access to an effective and accessible procedure allowing her to establish her entitlement to the medical services that her physical and mental condition required.”); CERD Committee, Concluding observations on the combined tenth to twelfth reports of the United States of America (U.N. Doc. CERD/C/USA/CO/10-12) (21 Sept. 2022), ¶¶ 35-36.
[193] See ICCPR, Art. 17; CRC, Art. 16.
[194] The Human Rights Committee has found violations of the right to privacy in every case it has considered when the State interfered with reproductive decision-making or abortion access. See HRC, Whelan v. Ireland, CCPR/C/119/D/2425/2014 (“Whelan v. Ireland”), ¶ 7.8; HRC, Mellet v. Ireland, CCPR/C/116/D/2334/2013 (“Mellet v. Ireland”), ¶ 7.7-7.8; HRC, K.L. v. Peru, CCPR/C/85/D/1153/2003 (“K.L. v. Peru”), ¶ 6.4; HRC, V.D.A. (on behalf of L.M.R.) v. Argentina, CCPR/C/101/D/1608/2007 (“V.D.A. v. Argentina”), ¶ 9.3; HRC, General Comment 28 (2000) on the equality of rights between men and women (U.N. Doc. CCPR/C/21/Rev.1/Add.10) (29 Mar. 2000), ¶ 20 (“States parties must provide information to enable the Committee to assess the effect of any laws and practices that may interfere with women’s right to enjoy privacy” such as “where States impose a legal duty upon doctors and other health personnel to report cases of women who have undergone abortion. . . . States parties should report on any laws and public or private actions that interfere with the equal enjoyment by women of the rights under article 17, and on the measures taken to eliminate such interference and to afford women protection from any such interference.”).
[195] See Whelan v. Ireland, ¶ 7.9; Mellet v. Ireland, ¶ 7.8; K.L. v. Peru, ¶ 6.4.
[196] Memorandum from Oklahoma Attorney General to All Oklahoma Law Enforcement Agencies on Guidance for Oklahoma law enforcement following Dobbs v. Jackson Women’s Health Org. (31 Aug. 2022), https://www.ok.gov/cleet/documents/Memo%20to%20Law%20Enforcement%20Following%20Dobbs%20(8.31.22).pdf.
[197] ICCPR, Art. 19.
[198] See, e.g., Whelan v. Ireland, ¶ 7.5-7.7; Mellet v. Ireland, ¶ 7.4-7.6; K.L. v. Peru, ¶ 6.3; V.D.A. v. Argentina, ¶ 9.2; CAT Committee, Concluding observations on the sixth periodic report of the United Kingdom of Great Britain and Northern Ireland (U.N. Doc. CAT/C/GBR/CO/6) (7 June 2019), ¶¶ 46-47; CAT Committee, Concluding observations of the Committee against Torture - Paraguay (U.N. Doc. CAT/C/PRY/CO/4-6) (14 Dec. 2011), ¶ 22; CAT Committee, Concluding observations on the initial report of Timor-Leste (U.N. Doc. CAT/C/TLS/CO/1) (29 Nov. 2017), ¶ 34.
[199] See CAT, Art. 16; ICCPR, Art. 7; CRC, Arts. 19, 37; CRPD, Art. 15.
[200] See CAT Committee, Concluding observations on the seventh periodic report of Poland (U.N. Doc. CAT/C/POL/CO/7) (29 Aug. 2019), ¶ 33(d).
[201] See HRC, Report of the Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment (U.N. Doc. A/HRC/31/57) (5 Jan. 2016), ¶ 44 (“The denial of safe abortions and subjecting women and girls to humiliating and judgmental attitudes in such contexts of extreme vulnerability and where timely health care is essential amount to torture or ill treatment.”).
[202] CAT Committee, Concluding observations on the third periodic report of the Philippines (U.N. Doc. CAT/C/PHL/CO/3) (2 June 2016), ¶ 40(b) (urging the state to “[r]eview its legislation in order to allow for legal exceptions to the prohibition of abortions in specific circumstances such as when the pregnancy endangers the life or health of the woman, when it is the result of rape or incest and in cases of foetal impairment…”) (emphasis added).
[203] See K.L. v. Peru, ¶ 6.3; Mellet v. Ireland, ¶¶ 7.4-7.6; Whelan v. Ireland, ¶¶ 7.4-7.7.
[204] V.D.A. v. Argentina, ¶ 9.2. See also HRC, General comment No. 36, Art. 6: right to life (U.N. Doc. CCPR/C/GC/36) (3 Sept. 2019), ¶ 8 (“States parties must provide safe, legal and effective access to abortion where the life and health of the pregnant woman or girl is at risk, or where carrying a pregnancy to term would cause the pregnant woman or girl substantial pain or suffering, most notably where the pregnancy is the result of rape or incest or where the pregnancy is not viable.”) (emphasis added).
[205] CEDAW Committee, General recommendation No. 35 on gender-based violence against women, updating general recommendation No. 19 (U.N. Doc. CEDAW/C/GC/35) (26 July 2017), ¶ 18.
[206] See ICCPR, Art. 9.
[207] HRC, Report of the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health (U.N. Doc. A/HRC/38/36) (10 Apr. 2018), ¶ 75.
[208] HRC, Concluding observations on the seventh periodic report of El Salvador (U.N. Doc. CCPR/C/SLV/CO/7) (9 May 2018), ¶ 16.
[209] See supra ¶¶ 22-23 on “fetal personhood” approaches.
[210] See supra ¶ 22.
[211] HRC, Report of the Working Group on Arbitrary Detention on its visit to the United States of America (U.N. Doc. A/HRC/36/37/Add.2) (17 July 2017), ¶¶ 73-74 (Detention on discriminatory grounds is defined as arbitrary). See HRC, Rep. of the Working Grp. on Arbitrary Det., Annex (U.N. Doc. A/HRC/16/47) (19 Jan. 2011), p. 23, ¶ 8(e). See also OHCHR, “Working Group on Arbitration Detention: About Arbitrary Detention”, available at https://www.ohchr.org/en/about-arbitrary-detention (clarifying that the definition of arbitrary detention under the Working Group’s mandate includes “deprivation[s] of liberty [which] constitute[] a violation of the international law for reasons of discrimination based on…gender,…disability; or other status….”).
[212] See ICCPR, Art. 18.
[213] HRC, General Comment No. 22: Article 18 (Freedom of Thought, Conscience or Religion) (U.N. Doc. CCPR/C/GC/22) (20 July 1993), ¶ 4.
[214] HRC, Report of the Special Rapporteur on freedom of religion or belief, Heiner Bielefeldt (U.N. Doc. A/HRC/71/269/) (28 Dec. 2016), ¶ 15.
[215] The HRC is clear that the concept of “morals” derives from many social, philosophical and religious traditions; consequently, limitations on the freedom to manifest a religion or belief for the purpose of protecting morals must be based on principles not deriving exclusively from a single tradition. HRC, General Comment No. 22: Article 18 (Freedom of Thought, Conscience or Religion) (U.N. Doc. CCPR/C/GC/22) (30 July 1993), ¶ 8. In its general comment on freedom of expression which contains a similar limitation clause, the HRC reiterated this and outlined that interpretation of morality should comply with the conception of human rights as ‘universal’, with particular emphasis on the standard of non-discrimination. See also HRC, General Comment No. 34: Art. 19 (Freedoms of opinion and expression) (U.N. Doc. CCPR/C/GC/34) (12 Sept. 2011), ¶ 32; HRC, General Comment No. 37: Article 21 (Right of peaceful assembly) (U.N. Doc.CCPR/C/GC/37) (17 Sept. 2020), ¶ 46.
[216] Id.
[217] Id.; HRC, Freedom of religion or belief: Report of the Special Rapporteur on freedom of religion or belief (U.N. Doc. A/HRC/40/58) (5 Mar. 2019), ¶ 17.
[218] See HRC, General Comment No. 34: Art. 19 (Freedoms of opinion and expression) (U.N. Doc. CCPR/C/GC/34) (12 Sept. 2011), ¶ 25.
[219] See supra Section I(B).
[220] See supra Section I(B) on the human rights implications of criminal abortion laws in the US.
[221] See supra note 219, ¶ 34 (Outlining that the grounds for restriction “must be appropriate to achieve their protective function; they must be the least intrusive instrument amongst those which might achieve their protective function; they must be proportionate to the interest to be protected…The principle of proportionality has to be respected not only in the law that frames the restrictions but also by the administrative and judicial authorities in applying the law.”).
[222] See ICCPR, Arts. 2-3, 26; ICERD, Arts. 2, 5; CEDAW, Art. 12.
[223] See Mellet v. Ireland, ¶¶ 7.11, 3.19; Whelan v. Ireland, ¶ 7.12.
[224] CEDAW Committee, General Recommendation No. 24: Article 12 of the Convention (Women and Health) (U.N. Doc. A/54/38/Rev.1) (1999), ¶ 11 (“It is discriminatory for a State party to refuse to provide legally for the performance of certain reproductive health services for women.”).
[225] CEDAW Committee, Inquiry concerning the United Kingdom of Great Britain and Northern Ireland under article 8 of the Optional Protocol to the Convention on the Elimination of All Forms of Discrimination against Women (U.N. Doc. CEDAW/C/OP.8/GBR/1) (6 Mar. 2018), ¶ 74.
[226] Working Group on the issue of discrimination against women in law and in practice, Women’s Autonomy, Equality and Reproductive Health in International Human Rights: Between Recognition, Backlash and Regressive Trends (Oct. 2017), p. 2, https://www.ohchr.org/sites/default/files/Documents/Issues/Women/WG/WomensAutonomyEqualityReproductiveHealth.pdf.
[227] See supra ¶¶ 33-37.
[228] See ICERD, Arts. 2, 5. See also CERD Committee, Concluding observations on the combined tenth to twelfth reports of the United States of America (U.N. Doc. CERD/C/USA/CO/10-12) (21 Sept. 2022), ¶¶ 35-36.
[229] CERD Committee, Concluding observations on the combined tenth to twelfth reports of the United States of America (U.N. Doc. CERD/C/USA/CO/10-12) (21 Sept. 2022), ¶ 35.
[230] Id., ¶ 36.
[231] Mellet v. Ireland, ¶ 7.11.
[232] Id.
[233] Working Group on the issue of discrimination against women in law and in practice, Women’s Autonomy, Equality and Reproductive Health in International Human Rights: Between Recognition, Backlash and Regressive Trends (Oct. 2017), p. 2, https://www.ohchr.org/sites/default/files/Documents/Issues/Women/WG/WomensAutonomyEqualityReproductiveHealth.pdf.
[234] Id.
[235] CRC Committee, General Comment No. 20 on the implementation of the rights of the child during adolescence (U.N. Doc. CRC/C/GC/20) (6 Dec. 2016), ¶ 60.
[236] Id., ¶¶ 60-61 (finding that adolescent girls should have access to information about sexual and reproductive health along with access to adequate health services). See also CRC Committee, General Comment No.4: Adolescent health and development in the context of the Convention on the Rights of the Child (U.N. Doc. CRC/GC/2003/4) (1 July 2003), ¶ 13.
[237] See Office of the United Nations High Commissioner for Human Rights (OHCHR), Guiding Principles on Business and Human Rights: Implementing the United Nations “Protect, Respect and Remedy” Framework (HR/PUB/11/04) (2011), ¶ 11 (noting that “The responsibility to respect human rights is a global standard of expected conduct for all business enterprises wherever they operate. It exists independently of States’ abilities and/or willingness to fulfil their own human rights obligations….The responsibility of business enterprises to respect human rights is distinct from issues of legal liability and enforcement, which remain defined largely by national law provisions in relevant jurisdictions.”). See also Human Rights Watch, Federal Trade Commission Comment Re: Commercial Surveillance ANPR, R111004 (21 Nov. 2022).
[238] See supra Section I(C).
[239] See Statement, OHCHR, “Bachelet on US ruling on Dobbs v Jackson Women’s Health Organization” (24 June 2022), https://www.ohchr.org/en/statements/2022/06/bachelet-us-ruling-Dobbs-v-jackson-womens-health-organization.
[240] See Press Release, Special Procedures, “USA: UN experts denounce Supreme Court decision to strike down Roe v. Wade, urge action to mitigate consequences” (24 June 2022), https://www.ohchr.org/en/press-releases/2022/06/usa-un-experts-denounce-supreme-court-decision-strike-down-roe-v-wade-urge (Statement signed by the Working Group on discrimination against women and girls; the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health; the Special Rapporteur on violence against women, its causes and consequences; and endorsed by the Special Rapporteur on freedom of religion or belief; the Special Rapporteur on the rights of persons with disabilities; the Special Rapporteur in the field of cultural rights; the Special Rapporteur on trafficking in persons, especially women and children; the Special Rapporteur on contemporary forms of racism, racial discrimination, xenophobia and related intolerance; and the Special Rapporteur on the right to privacy). See also Center for Reproductive Rights, “Protecting Abortion Access in Europe – A Call to Action” (28 June 2022), https://reproductiverights.org/protecting-abortion-access-in-europe-a-call-to-action (“We are deeply concerned about the devastating consequences this regressive judgment will have for the lives, health and wellbeing of people across the United States.”); Brief of the United Nations Mandate Holders as Amici Curiae, Dobbs v. JWHO., 142 S. Ct. 2228, pp. 31-33 (2022), https://www.supremecourt.gov/DocketPDF/19/19-1392/193045/20210920163400578_19-1392%20bsac%20United%20Nations%20Mandate%20Holders.pdf (“Overturning or curtailing constitutional protections to abortion access established in Roe and Casey constitutes retrogression in violation of human rights law.…Dismantling the U.S. framework that has protected abortion access for nearly 50 years will lead to further violations of women’s and girls’ human rights.”).
[241] World Health Organization [WHO], Abortion Care guideline (8 Mar. 2022), https://www.who.int/publications/i/item/9789240039483.
No comments:
Post a Comment